Abstract: Advances in regenerative dentistry have significantly improved the management of bone deficiencies present at, or resulting from, tooth extraction when implant placement or other prosthetic restoration is planned. The integration of biologic mediators, osteoconductive scaffolds, and resorbable barrier membranes has contributed to more predictable regenerative outcomes in appropriately selected cases. Growth factor–enhanced matrices may provide complementary biologic and structural properties that support site development. Xenografts offer long-term volumetric stability, while allografts demonstrate more active remodeling potential; when combined with biologic stimulation, these materials are intended to enhance angiogenesis, cellular recruitment, and graft incorporation. This article reviews the biologic mechanisms, clinical applications, and handling characteristics of these regenerative materials from clinical, radiographic, and histologic perspectives. When used individually or synergistically they support predictable hard- and soft-tissue regeneration, optimize implant site development, and enhance long-term implant stability and esthetic outcomes.
Regenerative therapy has become integral to contemporary periodontal and implant-related treatment planning. As implant dentistry has evolved toward earlier placement protocols and prosthetically driven site development, the demand for predictable hard- and soft-tissue regeneration has increased correspondingly. Rather than simply replacing missing teeth, clinicians today are reconstructing biologic foundations capable of supporting long-term function and esthetics. Regenerative techniques allow for preservation of ridge volume following tooth extraction, regeneration of lost periodontal support around natural dentition compromised by disease, and reconstruction of alveolar defects.
Regeneration becomes particularly important when implant placement is planned in sites undergoing extraction or in areas presenting with residual ridge deficiencies from prior healed extractions. After tooth removal, physiologic remodeling results in horizontal and vertical dimensional loss of the alveolar ridge. Without intervention, this remodeling can compromise ideal implant positioning, prosthetic emergence profiles, and long-term peri-implant stability. Similarly, periodontal bone loss alters both structural support and vascular architecture, reducing the regenerative potential of the site unless biologic enhancement strategies are incorporated.1

S Series Implant Portfolio
Traditional grafting approaches utilizing autogenous or allogeneic bone have historically relied on osteoconduction, with variable osteoinductive contribution. While autogenous bone remains the gold standard due to its inherent cellular viability and growth factor content, donor site morbidity and limited availability restrict its routine use. Allogeneic bone matrices provide a biologically familiar scaffold but demonstrate variability in remodeling kinetics depending on mineralization and processing. Xenogeneic materials, particularly anorganic bovine bone mineral (ABBM), have demonstrated long-term volumetric stability; however, histologic analyses consistently show slow resorption and prolonged particle persistence.2 Although the structural stability provided by these methods is advantageous for space maintenance, the materials may lack intrinsic biologic signaling necessary to actively stimulate cellular recruitment and angiogenesis.
The development of bioactive mediators such as recombinant human platelet-derived growth factor-BB (rhPDGF-BB) and advanced collagen matrices has shifted regenerative therapy from passive scaffold placement toward biologically orchestrated tissue regeneration. rhPDGF-BB promotes chemotaxis, mitogenesis, and angiogenesis—events fundamental to early wound healing and osseous regeneration. When combined with osteoconductive scaffolds, growth factor therapy enhances cellular migration into the grafted site, accelerates vascular ingrowth, and supports more rapid conversion of graft material to vital host bone.3 The integration of biologic stimulation with mechanical scaffold stability reflects an evolution in regenerative strategies.
Human allograft matrices, xenogeneic scaffolds, collagen barriers, and growth factor systems are no longer viewed as independent modalities but rather as complementary components within a biologically driven regenerative strategy. Successful regenerative therapy requires creation of a protected microenvironment conducive to predictable tissue regeneration. Stability of the clot, exclusion of soft-tissue cells when indicated, angiogenic stimulation, and scaffold integrity collectively determine clinical success.4
This article reviews the biologic principles underlying regenerative materials, such as growth factor–enhanced matrices, xenogeneic scaffolds, and human allografts, and discusses their clinical applications and synergistic potential in implant site development. Case examples demonstrate, from a histologic perspective, the progressive incorporation and conversion of graft materials to viable host bone, reinforcing the importance of biologic enhancement combined with mechanical stability in achieving predictable implant-ready sites.
Human Bone Matrix for Ridge and Implant Site Development
Allograft bone has a long history of clinical use in periodontal and implant site development, with demineralized freeze-dried bone allograft (DFDBA) shown to remodel and be replaced by vital bone in periodontal and socket preservation applications when proper wound stability and exclusion of soft tissue are achieved.5-9 DFDBA is commonly used for socket preservation, ridge augmentation, guided bone regeneration (GBR) beneath barrier membranes, and sinus floor elevation, providing a biologically familiar scaffold.
Critical determinants of success with allografts include meticulous defect preparation, achieving and maintaining wound stability, and, when indicated, the use of a membrane to exclude epithelium and support the regenerative environment. Although demineralized allografts possess potential osteoinductive activity, this capability fluctuates based on donor and processing variables; clinicians should emphasize mechanical stability and biologic containment as primary drivers of clinical outcomes.10,11
Growth Factor–Enhanced Matrix
Combining rhPDGF-BB with a beta-tricalcium phosphate (β-TCP) scaffold creates growth factor–enhanced matrices that are designed to stimulate angiogenesis and tissue regeneration. The rhPDGF-BB growth factor stimulates the migration (chemotaxis) and proliferation (mitogenesis) of mesenchymal cells, osteoblasts, and fibroblasts. It can be mixed with or adsorbed onto an osteoconductive scaffold for cellular infiltration and extracellular matrix deposition.
This rhPDGF-BB-based regenerative therapy combined with β-TCP scaffold is applicable for the treatment of periodontal defects, gingival recession, and ridge augmentation, as well as for socket preservation, GBR, and treatment of peri-implant defects.12 A multicenter randomized controlled trial demonstrated significantly greater clinical attachment gain and bone fill in infrabony periodontal defects treated with a growth factor–enhanced matrix compared to β-TCP alone.13
Xenogeneic Scaffold for Bone Regeneration
ABBM is designed to maintain the trabecular architecture of human bone. This material’s porosity supports vascular infiltration (angiogenesis) and osteoconduction while maintaining long-term volume stability. It can serve as a biologically inert scaffold that gradually integrates with the adjacent host bone via creeping substitution. The material is indicated for socket and ridge preservation, sinus elevation, peri-implant regeneration, and periodontal defect repair. Histologic analyses have shown that ABBM facilitates new bone formation of 25% to 35% within 6 to 9 months while preserving graft volume and supporting long-term implant survival.14
Case Examples
Case 1
A 62-year-old male patient was referred for evaluation of bone loss on the maxillary left second molar (tooth No. 15) and to address the missing maxillary left first molar (tooth No. 14). Radiographically, a large defect was noted at the missing first molar related to the prior extraction of that tooth with adjacent bone loss on the mesial root of the second molar (Figure 1).
A treatment plan was formulated that required site grafting to augment the defect at the first molar site and resectioning and grafting the mesial root of the second molar. This would include periodontal grafting/regeneration around the remaining portion of the second molar with subsequent implant placement at the No. 14 site following site healing.
The patient presented for the surgical appointment. Blood was drawn to create leukocyte platelet-rich fibrin (L-PRF) for subsequent graft use. A crestal incision was made and a flap was elevated to expose the deficient alveolar site and second molar. The mesiobuccal root was sectioned from the rest of the tooth and extracted leaving the remaining tooth in place. The defect was debrided, confirming a small sinus communication present at the apical area where the second molar mesiobuccal root had been. The exposed dentin on the second molar was treated with ethylenediaminetetraacetic acid (EDTA) (KometaBio, kometabio.com) to improve the chances of developing a new periodontal attachment.15 L-PRF was mixed with demineralized cortical fibers (vallos®, Geistlich, geistlich-na.com), and mineralized cortical bone and deproteinized ABBM (Bio-Oss®, Geistlich) were hydrated in rhPDGF-BB to form a putty. The graft was placed into the root resection socket to shape the deficient ridge to ideal contour. An amnion-chorion membrane (BioXclude®, Solvita, solvita.org) was placed over the grafted sites and buccal aspect of the ridge and then covered with PRF. The flap margins were reapproximated to attempt primary closure and fixated with sutures (Prolene™, Ethicon, jnj.com).
The patient was seen at 9 months post-grafting to evaluate healing in preparation for implant placement. Radiographically, the graft blended with the adjacent host bone, and the bone loss on the mesial of the second molar was repaired (Figure 2). There appeared to be a normal-dimension periodontal ligament on the second molar up to the furcation where the root resection had been performed. Clinically, the ridge volume appeared wider and higher apicocoronally, although a slight area of bone was missing in the region where the mesiobuccal root of tooth No. 15 would have been located. Sufficient volume was created in the grafted sites to enable ideal implant placement.
A crestal incision was made, enabling flap elevation to expose the area. The ridge was filled with dense bone. A core sample was taken at the planned implant site with a 3.5-mm trephine drill and sent for histological analysis. An osteotomy was completed, and an implant was placed and a cover screw inserted. The flap was closed primarily and sutured. A radiograph was taken to document implant placement relative to the adjacent anatomy (Figure 3).
Histologic analysis: The core sample was prepared and sectioned, then dyed with Stevenel’s blue and Van Gieson’s picric fuchsin. A high-power, 100x histological image showed fragments of bone trabeculae and very few small remaining particles of xenograft that were not fused together by osteoid (Figure 4). The bone appeared to be vital with some new bone formation. There were no residual particles of the demineralized cortical fibers or the mineralized allograft placed. The marrow appeared to have fibrotic spaces. Adipose tissue and clear, empty spaces were present. The atypical appearance of this tissue in comparison with the other areas may represent an area of artifact—tissue damage during processing. Another view at 200x magnification (Figure 5) showed green-staining collagen tissue, in which fibroblasts were present.
In the upper left portion of Figure 4, an aggregation of small, dark, blue-staining inflammatory cells (lymphocytes) was present. In the upper right part of the image, around the two small pieces of xenograft, osteoblasts could be seen in the surrounding osteoid, but this was not observed clearly in other areas of the bone graft. The bone appeared to be vital bone with very little new bone formation on the peripheral area. There appeared to be no evidence of either the mineralized or demineralized allograft. A greater proportion of vital bone may support favorable periodontal and implant outcomes.
At 9 months post–implant placement the patient was seen for uncovering. A radiograph was taken, revealing that the bone graft had blended with the surrounding bone at the crestal level with the implant’s platform. The graft on the mesial of the second molar was stable, and there was no bleeding on probing. A full-thickness flap was elevated to expose the implant’s cover screw. After determining appropriate stability of the implant, a healing abutment was placed and the flap sutured. A radiograph was taken to verify healing abutment seating relative to the implant’s platform (Figure 6).
Two weeks later the site was scanned for fabrication of the restoration. A final restoration—a long-term transitional crown on the second molar—was placed on the implant so as to not disturb the new periodontal attachment subgingivally (Figure 7).
The patient at the time was being treated for diabetes, high blood pressure, and a thyroid condition, and considering his medical issues and medications he was at risk for poor surgical healing as well as a relatively high degree of susceptibility to inflammation, infection, and bone loss. Clinically, the flaps that were closed and sutured passively did not remain so in one small area. This could have allowed bacteria to penetrate into the coronal portion of the surgical site leading to early breakdown of the barrier, inflammation in the tissues, and poorer bone quality in that small area. This did not affect placement, restoration, or ideal maintenance of the implant placed in that site nor periodontal regeneration around the adjacent tooth. Both the lower bone quality and histologic presence of inflammation were noted to a significantly higher extent in this patient than in the other patient highlighted in this article (described in Case 2), who was treated with the same grafts and growth factors.
This case highlights the importance of clinicians knowing their patients, including their medical history, and following healing radiographically, not just clinically. It also illustrates the potential value of histologic analysis of regenerated material retrieved from treated sites in different patients.
Case 2
A 72-year-old female patient presented on referral with a failing mandibular left second molar (tooth No. 18) that had led to significant bone loss and a hopeless prognosis of the adjacent third molar (tooth No. 17) (Figure 8). Probing and mobility confirmed that the second molar was severely periodontally involved, and extraction was recommended. The patient was informed that implants could be placed to replace the missing first molar and the second molar, and socket, periodontal, and ridge augmentation grafting would be needed at the time of extraction of the second molar. If ideal healing were to occur, the third molar tooth might be able to be maintained along with the implants being placed.
Blood was drawn from the patent to create L-PRF. The second molar was extracted atraumatically. A crestal incision was made at the first molar site and a full-thickness flap was elevated to expose the area being treated. The socket was curetted to debride it, and the periodontally affected sites around the third molar were root planed and treated with EDTA. The third molar was missing more than 75% of mesial bone and had a deep buccal furcation involvement; either of these conditions alone led to a poor-to-hopeless prognosis. A graft of demineralized cortical fibers (vallos) was mixed with mineralized cancellous allograft and ABBM (Bio-Oss), which had been hydrated in rhPDGF-BB. This was then mixed with 10% calcium sulfate. This mixture was hydrated in and mixed with different preparations of L-PRF to create a “block” of bone (ie, “sticky” bone).
The graft mixture was placed to fill the extraction socket and the defect on the mesial and buccal surfaces of the third molar and augment the ridge at the missing first molar site to ideal contour. A barrier membrane (BioXclude) was placed around the graft on the mesial and buccal aspects of the third molar. A collagen barrier membrane (OSSIX Plus, Dentsply Sirona, dentsplysirona.com) was placed over the ridge at the first and second molar sites. The flap margins were reapproximated to attain primary closure and secured with polytetrafluoroethylene (PTFE) sutures. A radiograph was taken to document site grafting relative to the adjacent anatomy and tooth (Figure 9). The sutures were removed at 4 weeks and the healing was uneventful.
At 11 months post-extraction and socket grafting, the site appeared clinically ready to proceed with implant placement at the first and second molar sites. A cone-beam computed tomography (CBCT) and periapical radiograph (Figure 10) were taken to evaluate the grafted area and demonstrated a homogenous appearance of the graft with the surrounding host bone. Full volume was obtained and maintained in the appropriate locations to enable ideal implant placement. The site was flapped after a crestal incision, enabling full-thickness flap elevation. The crest presented with fill of the site and blending of the graft combination with the host’s bone. A core sample was taken at the second molar site using a 3.5-mm trephine drill to be sent for histological analysis. Osteotomies were completed and implants placed at the first and second molar sites (Figure 11). The flaps were reapproximated to obtain primary closure following placement of cover screws on the implants and then sutured.
Histologic analysis: The core sample following sectioning and staining with Stevenel’s blue and Van Gieson’s picric fuchsin dyes revealed 81% bone, which was 100% vital and 18% marrow or fibrous tissue. Histologic sections demonstrated apparent resorption of mineralized graft components in these specimens. Those sites were replaced with vital bone, ideal for osseointegration and periodontal support. The percentage of vital bone observed in this case appears higher than that reported in some published studies; however, differences in methodology and patient variables limit direct comparison.2,16,17
Analyzed at medium power (40x magnification), very dense trabeculae with a good amount of vital cancellous bone was noted (Figure 12). New bone formation as well as bone remodeling and delicate marrow space was evident. As can be noted in Figure 12, different staining qualities reflected varying maturity levels of the different areas of the bone, with darker red-staining bone being less mature than the lighter-staining bone.
At higher magnification (100x) (Figure 13), the sample revealed thick trabeculae with obvious remodeling. Active new bone formation was evident with green-staining osteoid seams along the edge of the vital bone and marrow space, with osteocyte observed within the newly formed bone. The histologic appearance suggested advanced remodeling and maturation, especially for the posterior mandible and for a woman of advanced age. The graft materials were completely eliminated and replaced by vital bone. Figure 13 shows the different features of the healed bone and residual osteoclasts, which would have been responsible for removal of the mineralized components of the initial bone replacement graft material. This level of bone maturation may support favorable osseointegration in the first and second molar sites and periodontal regeneration around and improvement in prognosis of the third molar.
The patient presented at 8 months post–implant placement for exposure of the implants and initiation of the restorative phase of treatment. A periapical radiograph was taken to confirm ideal bone levels in relation to the implants’ platforms. The implants were exposed, cover screws were removed, and healing abutments were placed with PRF plugs to optimize soft-tissue healing and improve the thickness of the marginal gingiva. Due to a lower implant stability quotient (ISQ) measurement (Osstell, osstell.com) on the implant in site No. 18, electromagnetic healing abutments (MagDent, magdentmed.com) were used on both implants. A radiograph was taken to confirm seating of the abutments (Figure 14). Electromagnetic stimulation has been investigated as an adjunct to enhance implant stability; in this case, the electromagnetic healing abutment was used based on clinician preference.2 Additionally, the electromagnetic energy has been found to reduce the inflammatory activity of macrophages and the degradative activity of osteoclasts, stimulating bone regeneration around the implant.17 The soft tissue was reapproximated and sutured.
The patient returned 4 weeks later for impressions to begin restoration of the implants. The implant in the second molar site had improved in stability, potentially aided by the electromagnetic healing abutment.18-21 The restorations were returned from the dental laboratory and inserted. The bone level remained stable around the implants and third molar tooth throughout the first 18 months post-extraction and socket grafting (Figure 15).
At 10 months post–implant placement the patient was seen on recall. The gingival tissue around the implants presented with an absence of inflammation and a healthy appearance (Figure 16). Radiographically, bone remained stable around the implants with increased radiopacity around the implant in site No. 18 and no crestal changes (Figure 17) compared to the radiograph taken at implant placement (Figure 11).
Discussion
The integration of biologic mediators, bioactive membranes, and osteoconductive scaffolds has expanded regenerative therapy options in periodontal therapy and treatment of ridge defects and extraction sockets when planning implant placement. rhPDGF-BB promotes chemotaxis, mitogenesis, and angiogenesis—critical early events in osseous regeneration and site preparation. Mineralized xenografts provide microstructural stability and long-term volumetric maintenance through their slow resorption profile.
Human allograft matrices add another biologically relevant dimension to site development. Compared to xenogeneic matrices, human allograft demonstrates more active remodeling characteristics, which may contribute to earlier graft turnover and replacement with vital host bone when mechanical stability and soft-tissue containment are achieved.22 This can be particularly advantageous in socket preservation and contained ridge defects where accelerated integration is desirable prior to implant placement.
When utilized together, these materials appear to function synergistically. Growth factor stimulation from rhPDGF-BB accelerates early cellular events and vascular ingrowth, while either xenogeneic (eg, ABBM) or human allograft scaffolds maintain space and provide a matrix for bone deposition. The choice between xenograft and allograft becomes defect-driven and timeline-dependent: xenografts offer prolonged volumetric stability, whereas allografts may demonstrate more dynamic remodeling and turnover.23 Collectively, this biologically driven approach can enhance esthetic outcomes, may reduce healing intervals in selected cases, and could improve the long-term prognosis for implant placement and periodontal regeneration.
The choice of ABBM was validated in the present case reports, as it showed preserved scaffold architecture with gradual replacement by host bone. In these cases utilizing allograft matrices, graft particles demonstrated more active remodeling patterns with earlier replacement by viable bone. These findings are consistent with a defect-specific material selection strategy rather than a singular graft preference.
Ultimately, graft behavior must be interpreted within the context of biologic stimulus, scaffold stability, and wound management. No one material alone determines the final outcome; stability, vascularity, and containment remain the primary drivers of regenerative success.
Conclusion
The biologic and structural characteristics of growth factor–enhanced matrices, xenogeneic matrices, and human allografts may serve as complementary regenerative factors within a comprehensive treatment strategy. Growth factor–mediated cellular activation, combined with a stable osteoconductive scaffold and protected regenerative environment, may create favorable conditions for hard-tissue development when planning implant placement.
By integrating biologic stimulation, ie, rhPDGF-BB, appropriate scaffold selection of ABBM for long-term volumetric stability or allograft for enhanced remodeling, and resorbable, bioactive barrier membranes, clinicians can tailor regenerative therapy to a specific clinical scenario. These materials collectively represent the continued evolution of implant site development from passive grafting toward biologically orchestrated tissue regeneration. As demonstrated in the cases presented, when applied with meticulous surgical technique and sound case selection, this synergistic strategy can successfully achieve maintenance of ridge volume and vital bone formation for implant-supported restoration.
DISCLOSURE
Dr. Horowitz receives financial and material support from
Solvita and Geistlich. Dr. Kurtzman received an honorarium from Geistlich for writing this article.
About the Authors
Robert A. Horowitz, DDS
Adjunct Clinical Assistant Professor, Departments of Oral and Maxillofacial Surgery and Periodontology and Implant Dentistry, New York University College of Dentistry, New York, New York
Gregori M. Kurtzman, DDS, MAGD
Former Assistant Clinical Professor, University of Maryland School of Dentistry, Baltimore, Maryland; Private Practice, Silver Spring, Maryland
Hari S. Prasad, MS
Assistant Director, Hard Tissue Research Laboratory, Division of Oral and Maxillofacial Pathology, and Senior Research Scientist, University of Minnesota School of Dentistry, Minneapolis, Minnesota
References
1. Cortellini P, Tonetti MS. Clinical concepts for regenerative therapy in intrabony defects. Periodontol 2000. 2015;68(1):282-307.
2. Artzi Z, Tal H, Dayan D. Porous bovine bone mineral in healing of human extraction sockets. Part 1: histomorphometric evaluations at 9 months. J Periodontol. 2000;71(6):1015-1023.
3. Kaigler D, Avila G, Wisner-Lynch L, et al. Platelet-derived growth factor applications in periodontal and peri-implant bone regeneration. Expert Opin Biol Ther. 2011;11(3):375-385.
4. Wang HL, Boyapati L. “PASS” principles for predictable bone regeneration. Implant Dent. 2006;15(1):8-17.
5. Schwartz Z, Mellonig JT, Carnes DL Jr, et al. Ability of commercial demineralized freeze-dried bone allograft to induce new bone formation. J Periodontol. 1996;67(9):918-926.
6. Alshoiby MM, Fawzy El-Sayed KM, Elbattawy W, Hosny MM. Injectable platelet-rich fibrin with demineralized freeze-dried bone allograft compared to demineralized freeze-dried bone allograft in intrabony defects of patients with stage-III periodontitis: a randomized controlled clinical trial. Clin Oral Investig. 2023;27(7):3457-3467.
7. Paul BF, Horning GM, Hellstein JW, Schafer DR. The osteoinductive potential of demineralized freeze-dried bone allograft in human non-orthotopic sites: a pilot study. J Periodontol. 2001;72(8):1064-1068.
8. Mellonig JT. Decalcified freeze-dried bone allograft as an implant material in human periodontal defects. Int J Periodontics Restorative Dent. 1984;4(6):40-55.
9. Dhamija R, Tewari S, Narula SC, et al. Socket preservation with demineralized freeze-dried bone allograft and platelet-rich fibrin in humans: a randomized controlled clinical trial. J Craniomaxillofac Surg. 2020;48(10):938-947.
10. Glowacki J. A review of osteoinductive testing methods and sterilization processes for demineralized bone. Cell Tissue Bank. 2005;6(1):3-12.
11. Kothiwale S, Bhimani R, Kaderi M, Ajbani J. Comparative study of DFDBA and FDBA block grafts in combination with chorion membrane for the treatment of periodontal intra-bony defects at 12 months post-surgery. Cell Tissue Bank. 2019;20(2):225-235.
12. Alkindi M, Ramalingam S, Alghamdi O, et al. Guided bone regeneration with osteoconductive grafts and PDGF: a tissue engineering option for segmental bone defect reconstruction. J Appl Biomater Funct Mater. 2021;19:2280800020987405.
13. Nevins M, Giannobile WV, McGuire MK, et al. Platelet-derived growth factor stimulates bone fill and rate of attachment level gain: results of a large multicenter randomized controlled trial. J Periodontol. 2005;76(12):2205-2215.
14. da Silva HF, Goulart DR, Sverzut AT, et al. Comparison of two anorganic bovine bone in maxillary sinus lift: a split-mouth study with clinical, radiographical, and histomorphometrical analysis. Int J Implant Dent. 2020;6(1):17.
15. Zhan X, Wang X, Li J, et al. LPCGF and EDTA conditioning of the root surface enhances the biological behavior of human periodontal ligament stem cells. J Periodontol. 2021;92(2):301-311.
16. Vance GS, Greenwell H, Miller RL, et al. Comparison of an allograft in an experimental putty carrier and a bovine-derived xenograft used in ridge preservation: a clinical and histologic study in humans. Int J Oral Maxillofac Implants. 2004;19(4):491-497.
17. Artzi Z, Tal H, Dayan D. Porous bovine bone mineral in healing of human extraction sockets: 2. Histochemical observations at 9 months. J Periodontol. 2001;72(2):152-159.
18. Barak S, Matalon S, Dolkart O, et al. Miniaturized electromagnetic device abutment improves stability of the dental implants. J Craniofac Surg. 2019;30(4):1055-1057.
19. Trentini M, D’Amora U, Ronca A, et al. Bone regeneration revolution: pulsed electromagnetic field modulates macrophage-derived exosomes to attenuate osteoclastogenesis. Int J Nanomedicine. 2024;19:8695-8707.
20. Caliogna L, Medetti M, Bina V, et al. Pulsed electromagnetic fields in bone healing: molecular pathways and clinical applications. Int J Mol Sci. 2021;22(14):7403.
21. Yuan J, Xin F, Jiang W. Underlying signaling pathways and therapeutic applications of pulsed electromagnetic fields in bone repair. Cell Physiol Biochem. 2018;46(4):1581-1594.
22. Fretwurst T, Nelson K, Tarnow DP, et al. Is bone grafting and guided bone regeneration needed for dental implants? A critical review of the literature. J Periodontol. 2018;89(suppl 1):S144-S166.
23. Jensen SS, Bosshardt DD. Bone graft materials and biological mechanisms in sinus floor augmentation. Periodontol 2000. 2014;66(1):239-271.
Figures and Images
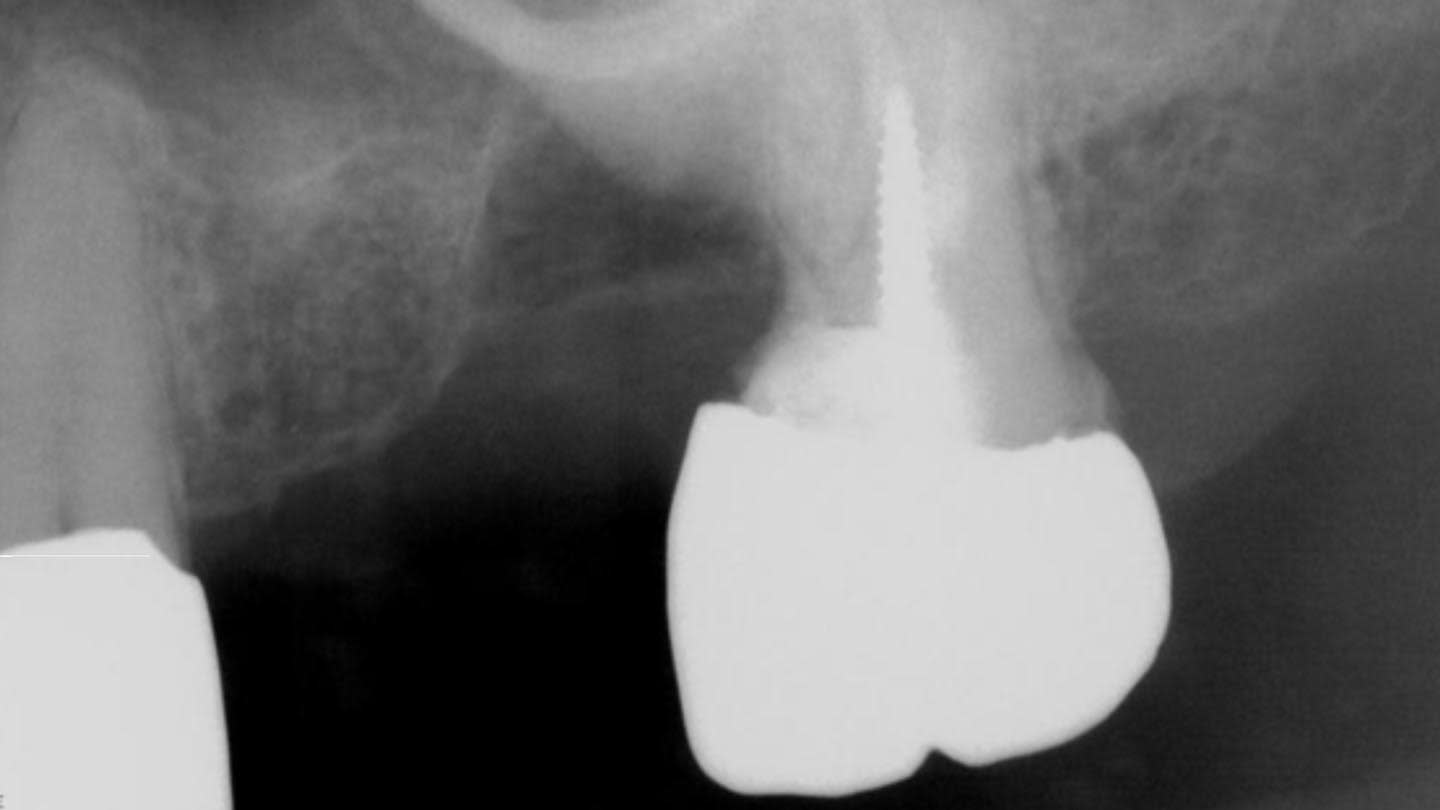
Figure 1

Figure 2

Figure 3

Figure 4
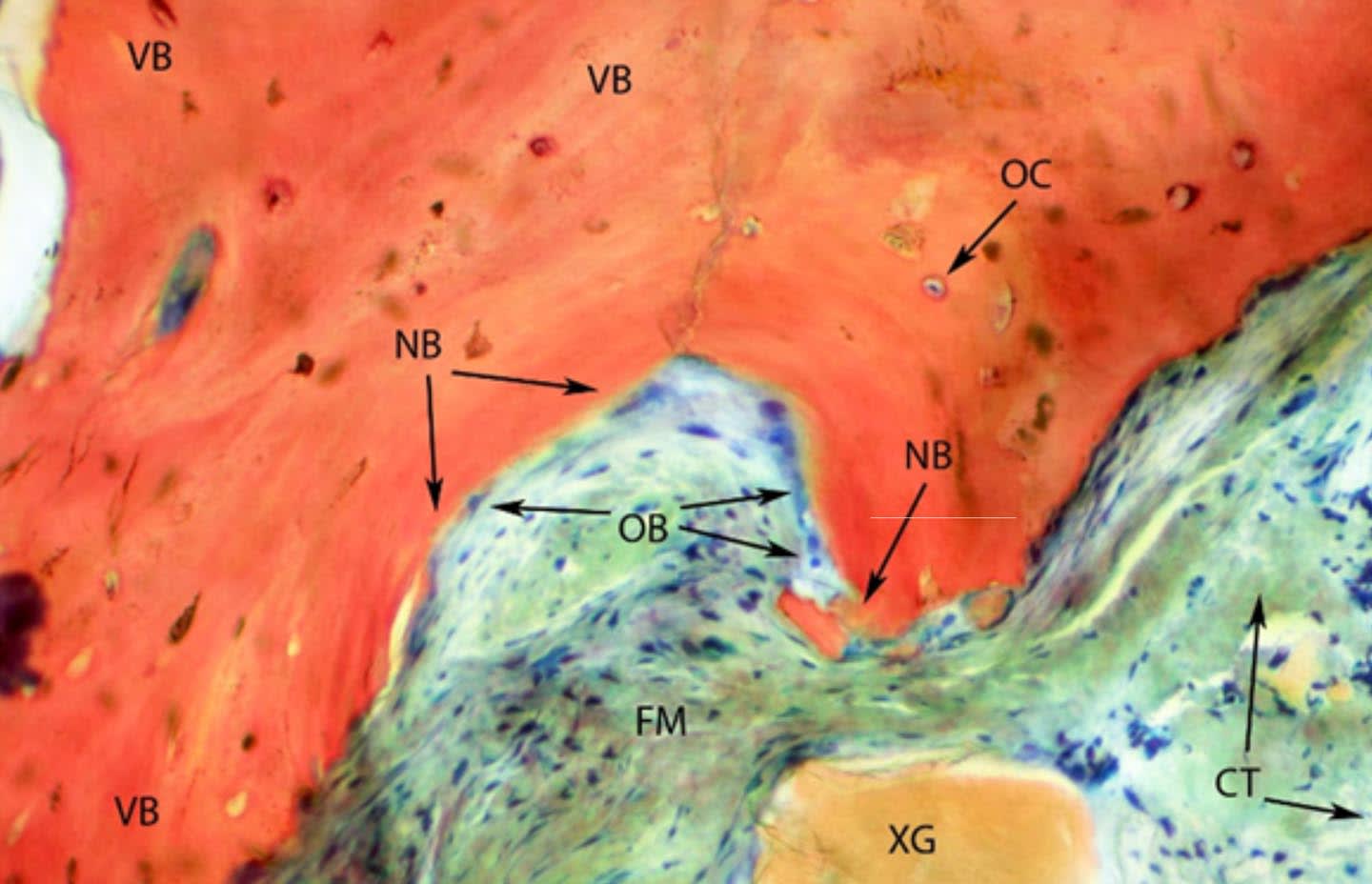
Figure 5

Figure 6
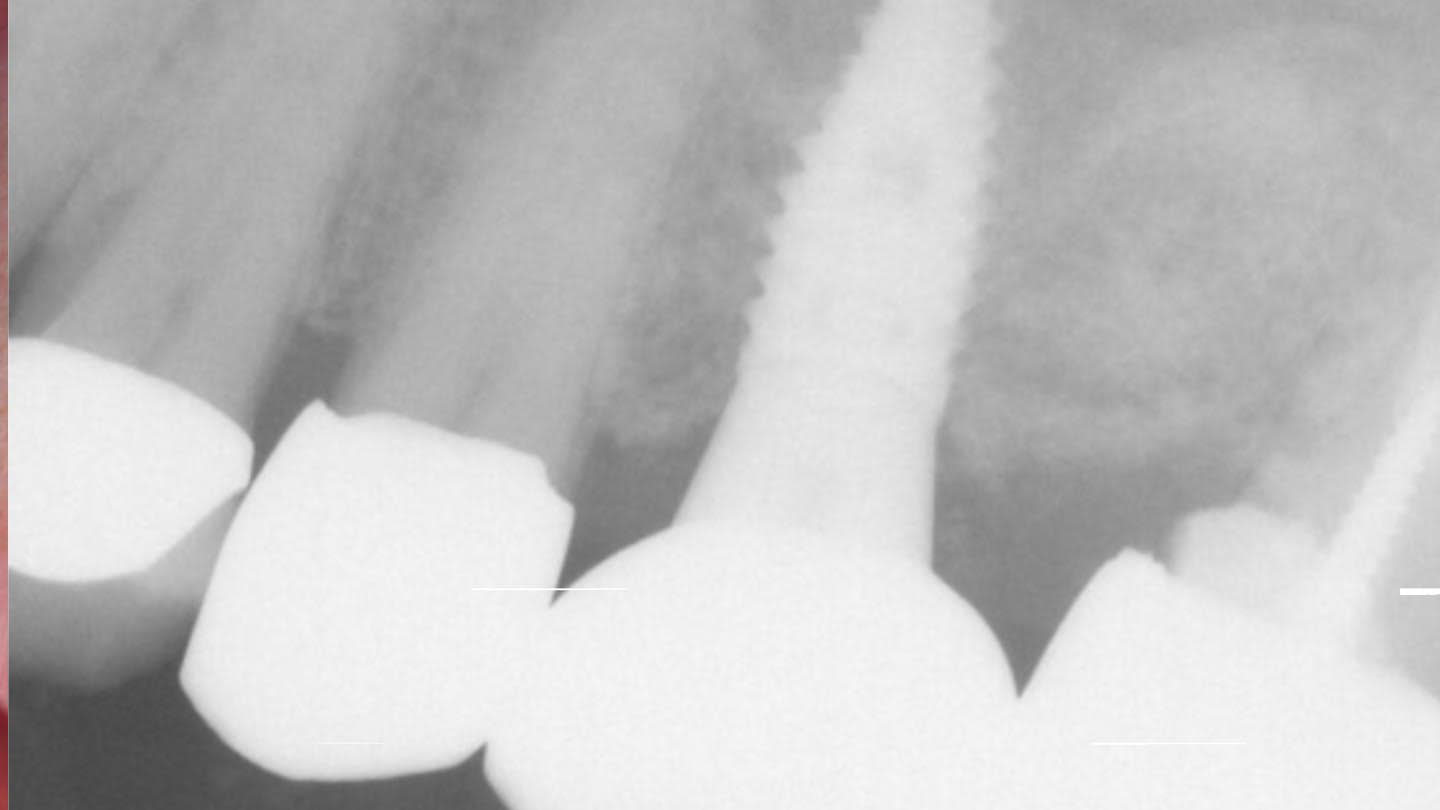
Figure 7

Figure 8
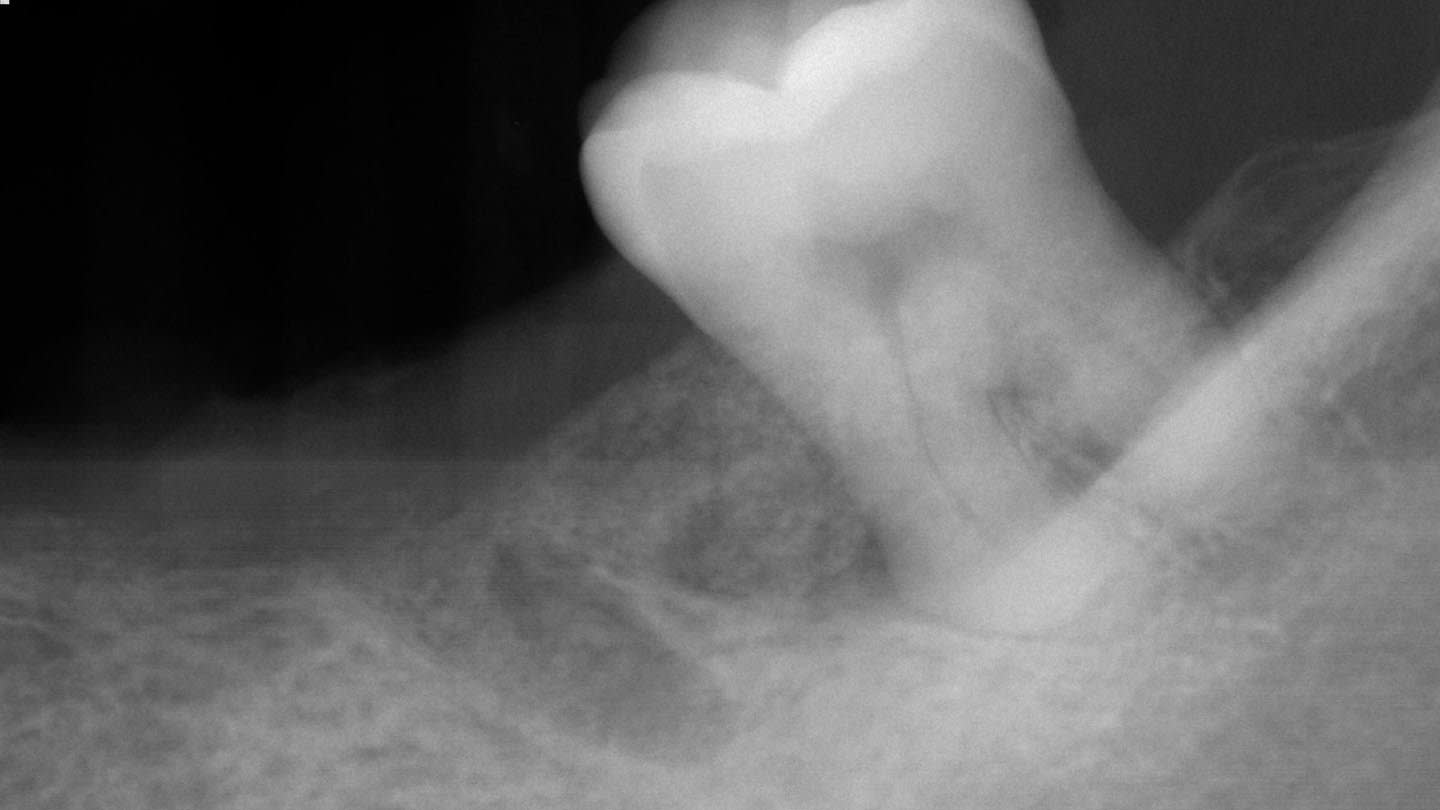
Figure 9
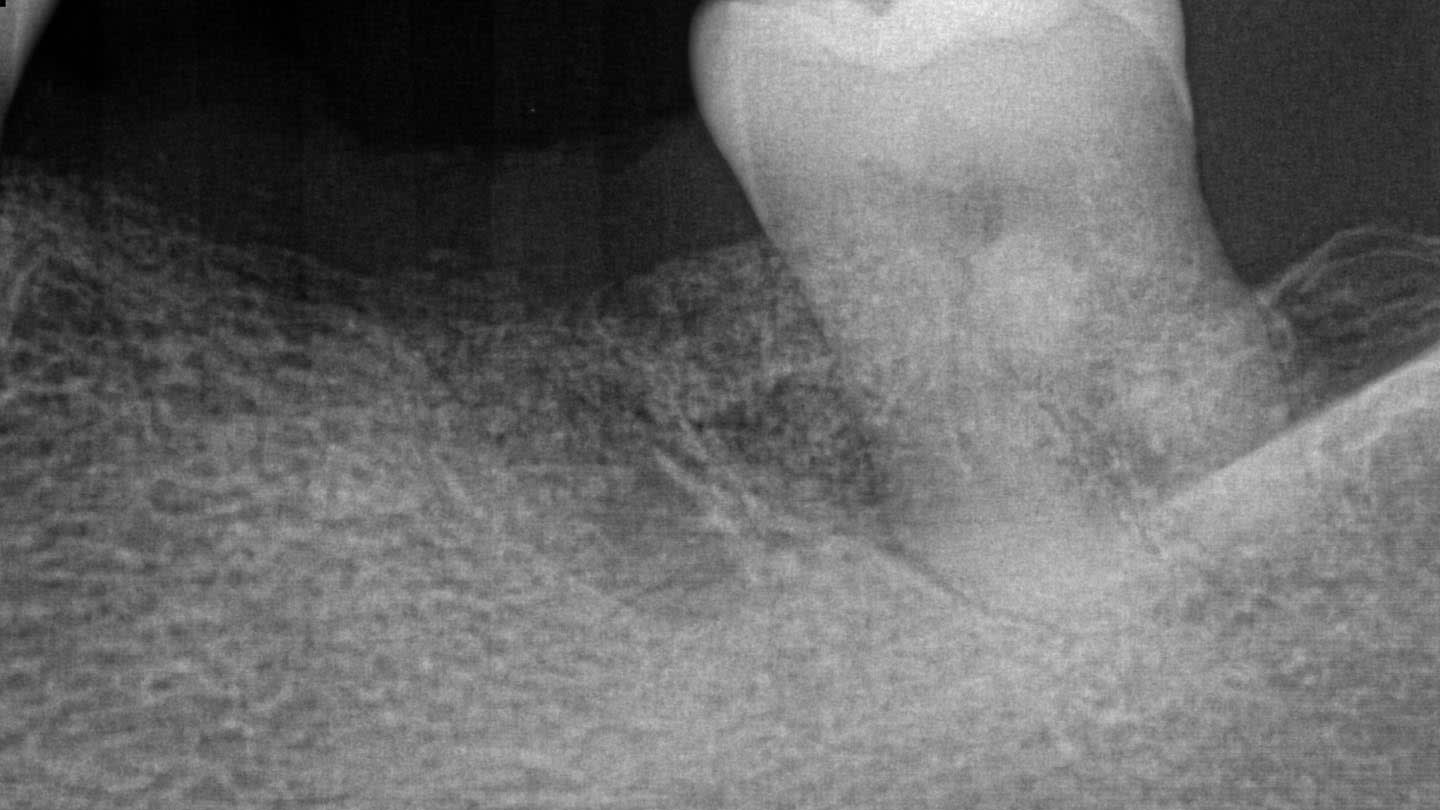
Figure 10
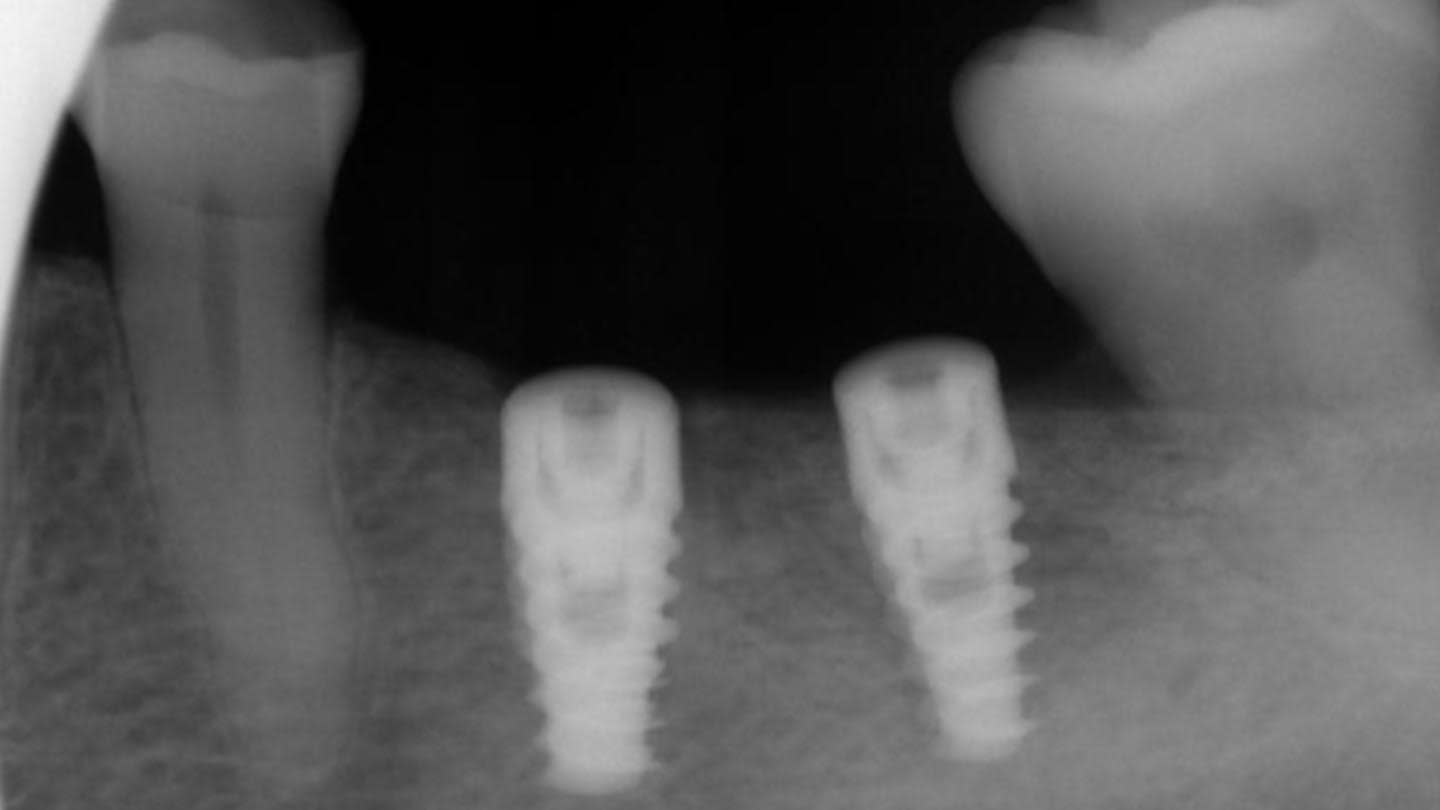
Figure 11
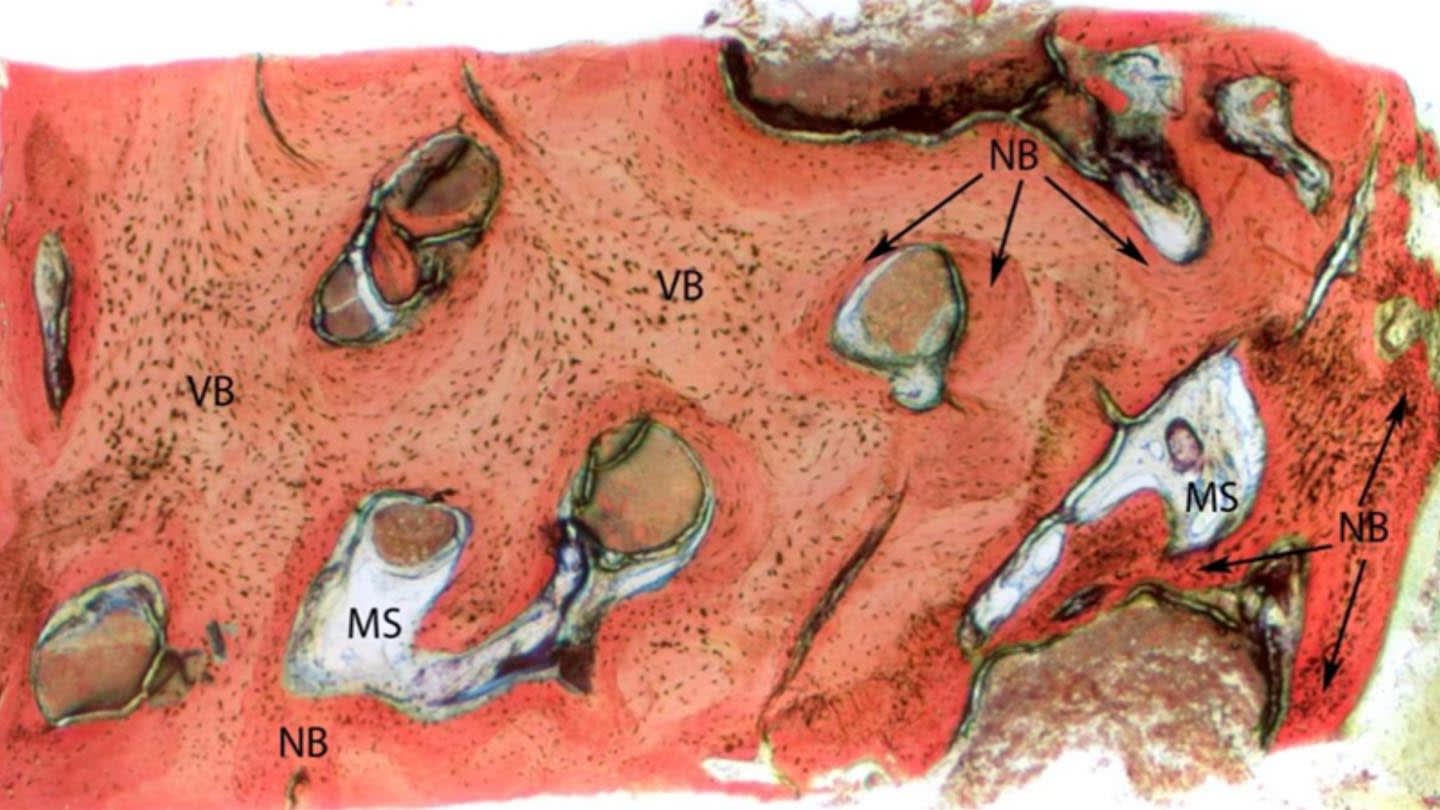
Figure 12
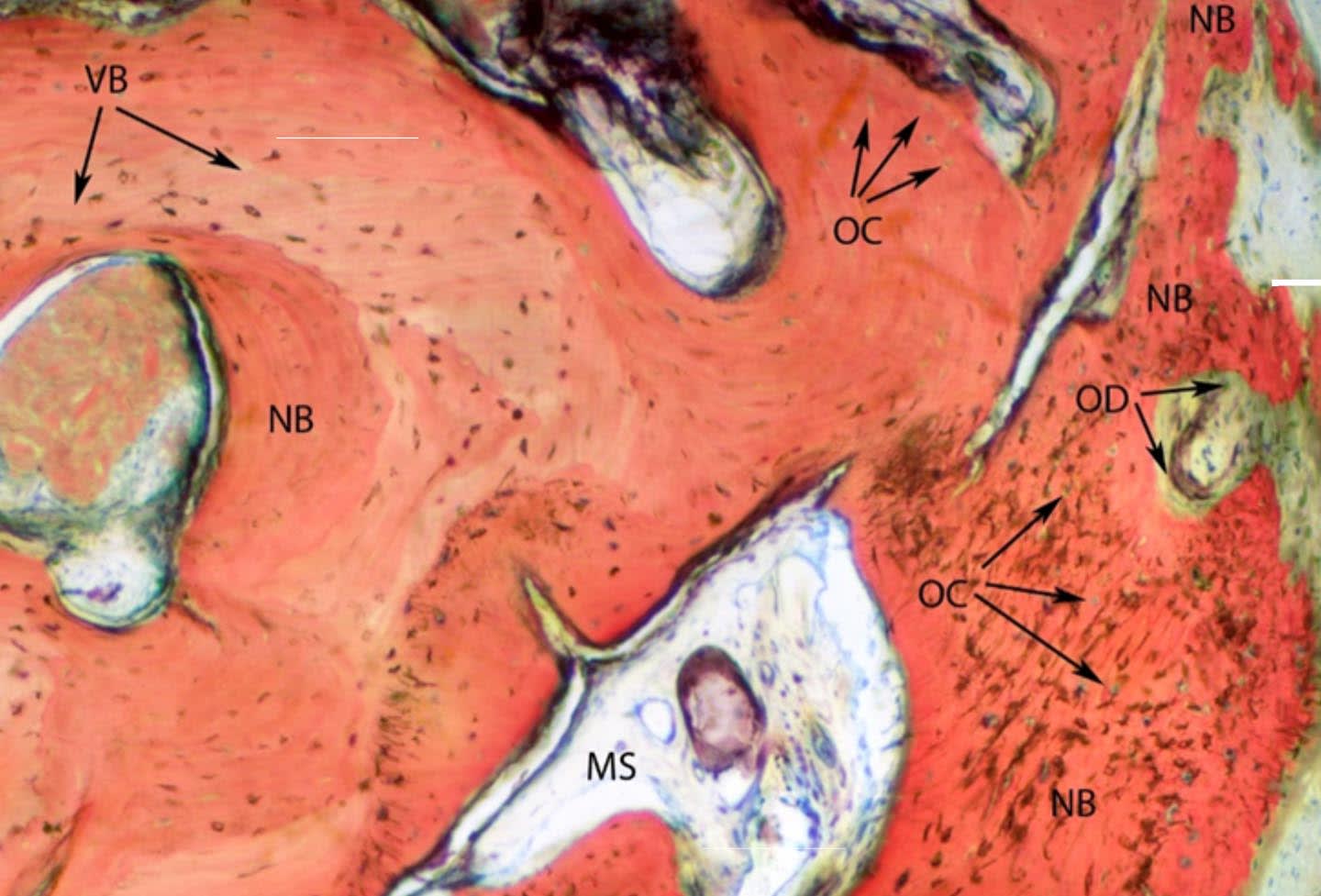
Figure 13
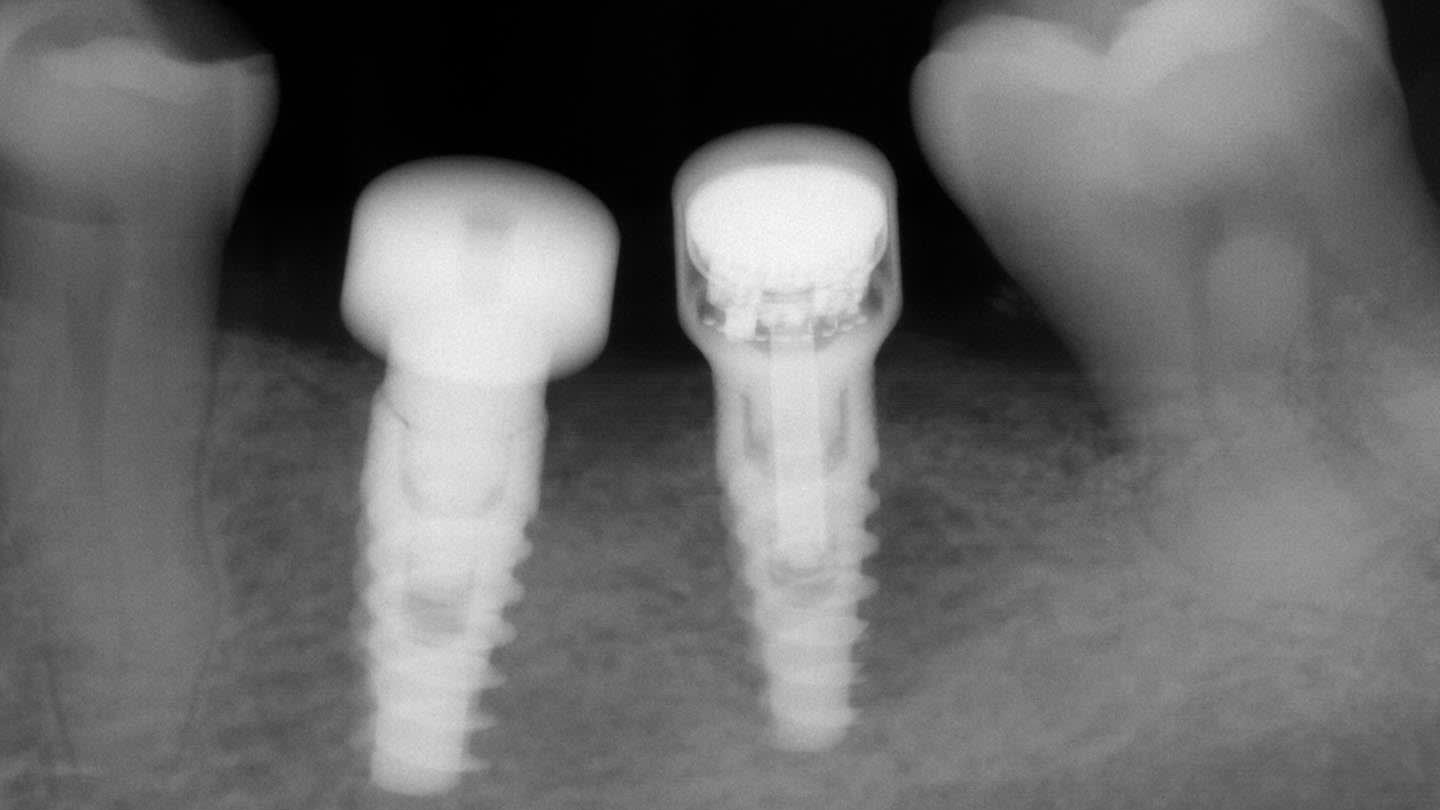
Figure 14
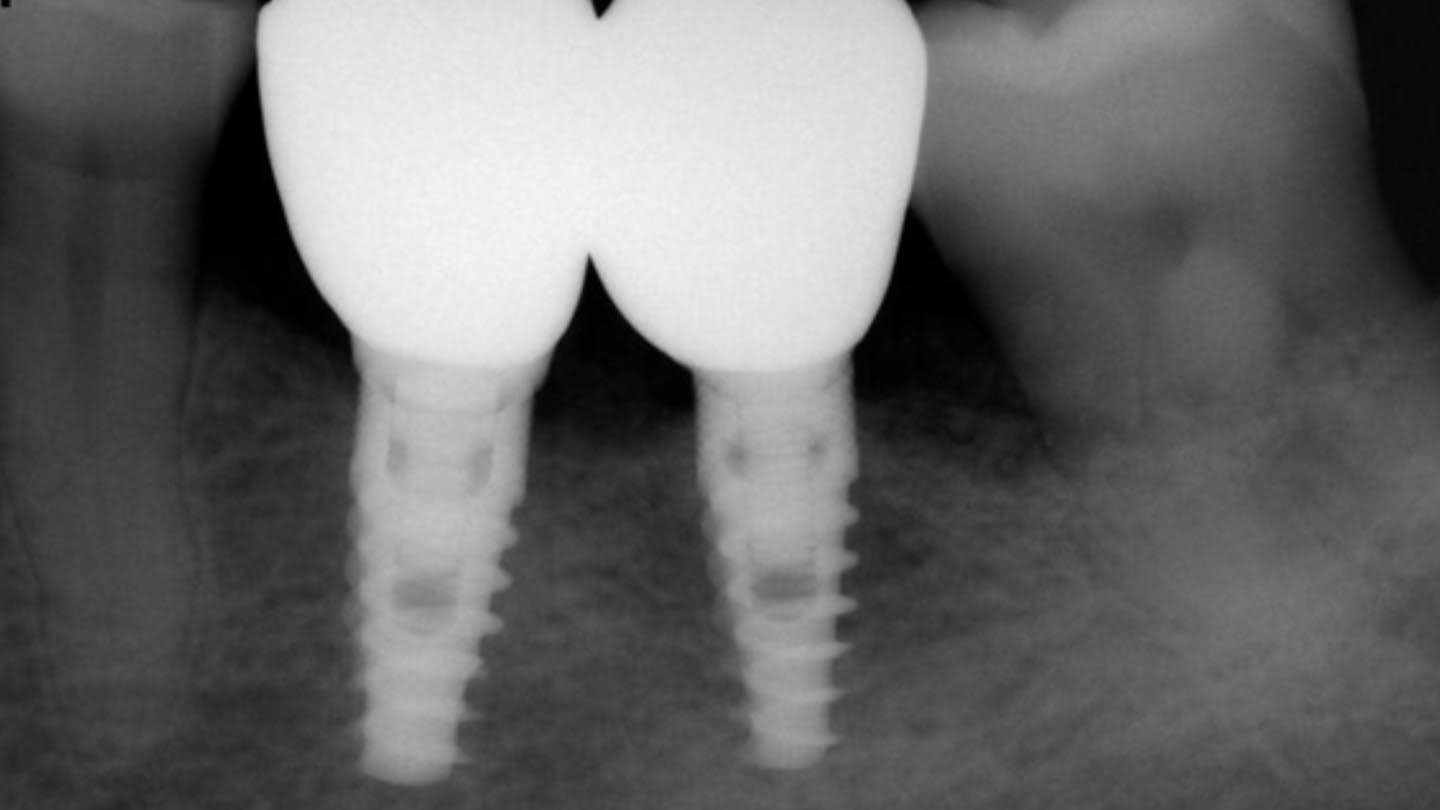
Figure 15

Figure 16
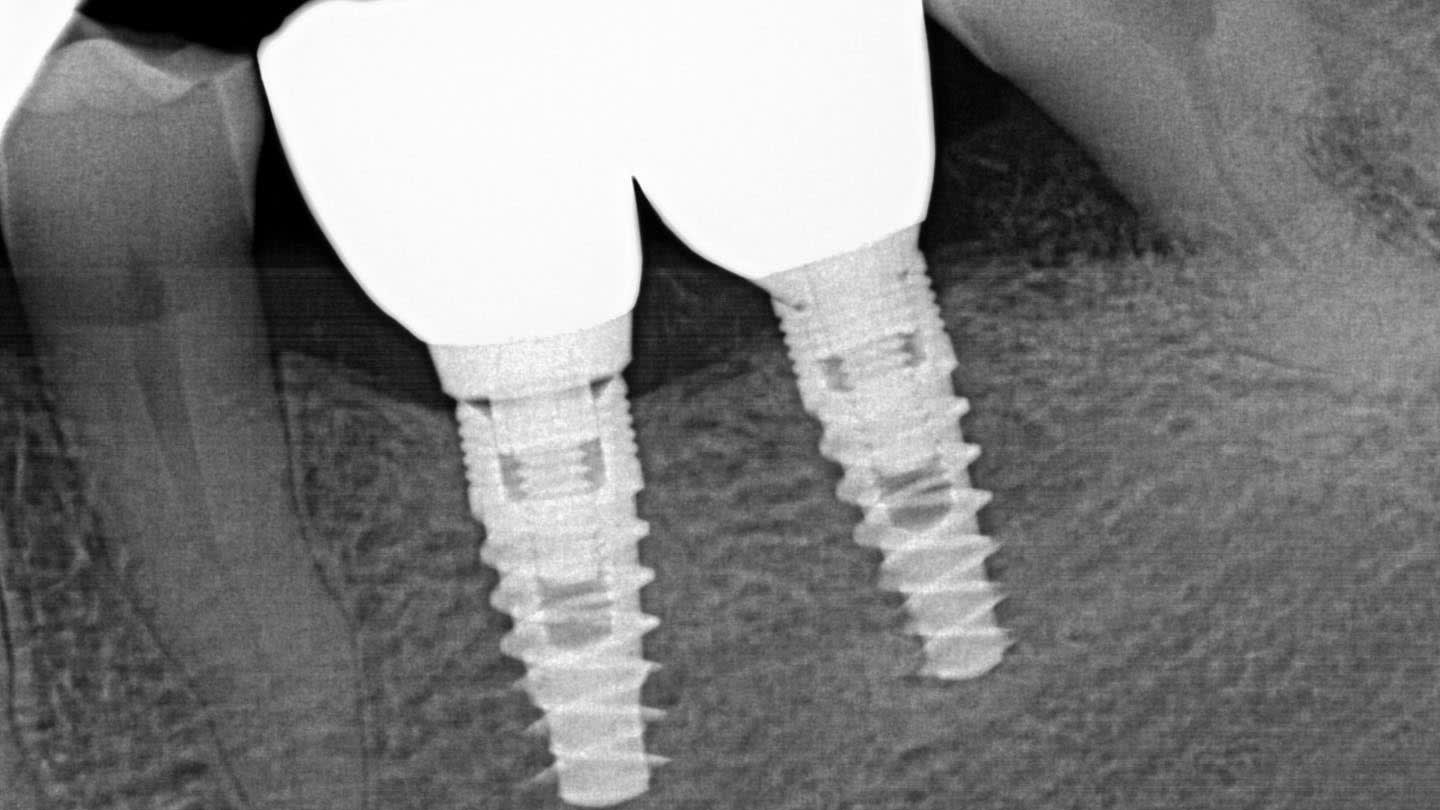
Figure 17
