The evolution of dental implants from an unvalidated mechanistic procedure to a clinically validated intervention has been driven by the integration of material sciences, tissue biology, and clinical expertise, culminating in a remarkable therapeutic innovation whose impact may be comparable to that of fluoride in the prevention of dental caries. The surgical placement of an implant, unfortunately, involves many of the same traits that contribute to dental neglect and subsequent tooth loss that necessitates implant placement: fear of intraoral injections of a local anesthetic, a surgical incision into soft tissue, use of a drill to remove bone, and postoperative pain for several days augmented by the inflammatory cascade. Effective regional anesthesia and judicious use of an anxiolytic medication can overcome patient reticence to having an implant procedure, but postoperative pain must still be managed to reduce the risks of opioid adverse events or triggering substance abuse.1,2 This article emphasizes safe and effective strategies to minimize postoperative pain with targeted approaches in the peripheral nervous system (PNS) to lessen the onset and intensity of pain, decrease the incidence of opioid adverse events, and mitigate the development of substance abuse.
Pain Management in the Wake of the Opioid Overdose Crisis
Dental implant placement results in injury to mucosal tissue in the peri-implant area and underlying bone, activating peripheral nerve endings to signal nociception and the release of peripheral mediators of the inflammatory cascade that contribute to tissue injury and modulate the reparative process.3 Scientific understanding of the neurobiology of pain, its molecular-genetic basis, and the wide variability in the physiologic and cognitive processes that influence the individual pain phenotype has increased remarkably over the past half-century (Figure 1),4 but the pharmacologic armamentarium used to manage acute pain still relies heavily on traditional drug classes such as aspirin-like drugs (including nonsteroidal anti-inflammatory drugs [NSAIDs] and acetaminophen), opioids, and corticosteroids to suppress acute pain and inflammation.3 While these drug classes are efficacious alone and additive in combination, their use is limited by their relative lack of safety when administered in high doses or taken chronically, inadvertently precipitating substance abuse.

S Series Implant Portfolio
The scientific quest for novel analgesics without the limitations of currently available drugs has a long history of failed targets, unexpected toxicity when used widely, eg, the COX-2 inhibitors, or delayed recognition of toxicity, eg, acetaminophen combined with alcoholic beverages. The recent opioid epidemic was largely attributed to pharmaceutical over-promotion and the wide availability of illicit fentanyl.5 Peaking in 2022, US drug overdose mortality declined substantially through 2024 and continued to show provisional decreases into 2025.6-10 Despite this encouraging downward trend, overdose deaths remain at historically elevated levels relative to pre-pandemic levels and continue to be driven predominantly by illicit synthetic opioids, particularly fentanyl, frequently in combination with stimulants.9,10 Deaths involving natural and semisynthetic opioids—a category that includes commonly prescribed opioid types—represent a smaller and declining proportion of total overdose mortality.9 Thus, the current status of overdose deaths in the United States reflects an improving but still significant public health crisis characterized primarily by illicit drug exposure but overlooks the exponential increase in substance abuse prior to the opioid overdose epidemic attributed to clinical pain management.11
Clinicians should recognize that substance abuse is endemic in American society, but no long-term solutions are apparent as social determinants and genetic risk factors drive the process. This suggests that clinicians will need to continue to manage acute dental pain with existing drug classes until new drugs are developed, evaluated in clinical trials, receive regulatory approval, and demonstrate clinical efficacy and safety in practice to improve on the limitations of currently available analgesics.3,12
Selectively Targeting Pain After Implant Placement
An important consideration for analgesic management is the magnitude and duration of the anticipated postoperative pain based on the level of tissue injury and the ability to block the pathway from the initiation of nociceptive signaling at the site of injury through the PNS and central nervous system (CNS) before the signal is perceived as pain in the CNS. This nociceptive signaling is further augmented by the inflammatory cascade in the periphery and neuronal modulators in the dorsal horn as part of the response to the tissue injury. Figure 2 shows a simplified schematic of the neuronal pathways, receptors, neurotransmitter, cytokines, and cellular mediators that interact to result in an aversive pain signal at the time of tissue injury that is augmented by the inflammatory process to persist as postoperative pain for several days following the initial tissue injury.13 For decades, pharmaceutical development has targeted increasingly selective receptors, neurotransmitters, and cytokines to attenuate neuron transmission without the adverse effects of opioids and aspirin-like drugs, largely without success as illustrated by the opioid overdose crisis and gastrointestinal bleeding caused by overuse of NSAIDs.3
The available literature suggests that postoperative pain following routine dental implant placement is generally mild to moderate in intensity, typically peaking within the first 24 to 48 hours and gradually declining over the subsequent postoperative days.14 A rationale for drug selection to minimize the use of opioids by first-line therapy with more effective and safer NSAIDs and acetaminophen is summarized in Table 1.12,15 (To view Table 1, “Comparison of Conventional Approaches to Preventive Strategies,” visit compendiumlive.com/go/cced2121.) A long-acting local anesthetic such as 0.5% bupivacaine can be administered as part of the procedure or at the conclusion of the procedure to block nociceptive input into the nervous system that otherwise increases pain sensitivity to result in hyperalgesia postoperatively.16 The NSAID should be administered shortly after the procedure to attenuate both COX-1 and COX-2 mediated pain at the site of soft-tissue injury.3 Acetaminophen can also be administered in combination with the NSAID to provide additive analgesia with minimal adverse effects.3,12 If these preventive measures are inadequate, administration of an opioid can be considered but will likely increase the incidence of adverse effects with minimal additive analgesia.3,15
Conclusion
Effective postoperative pain management following dental implant placement requires a balanced, evidence-based approach that prioritizes patient safety while minimizing opioid exposure. Preventive strategies using long-acting local anesthetics, NSAIDs, and acetaminophen can provide effective analgesia by targeting nociceptive and inflammatory pathways early in the postoperative period. As the profession continues to address the broader challenges of substance abuse and opioid-related harm, clinicians should emphasize multimodal, opioid-sparing protocols that optimize patient comfort and clinical outcomes.
References
1. Harbaugh CM, Nalliah RP, Hu HM, et al. Persistent opioid use after wisdom tooth extraction. JAMA. 2018;320(5):504-506.
2. Schroeder AR, Dehghan M, Newman TB, et al. Association of opioid prescriptions from dental clinicians for US adolescents and young adults with subsequent opioid use and abuse. JAMA Intern Med. 2019;179(2):145-152.
3. Hersh EV, Moore PA, Grosser T, et al. Nonsteroidal anti-inflammatory drugs and opioids in postsurgical dental pain. J Dent Res. 2020;99(7):777-786.
4. Woodcock J, Witter J, Dionne RA. Stimulating the development of mechanism-based, individualized pain therapies. Nat Rev Drug Discov. 2007;6(9):703-710.
5. Quinones S. Dreamland: The True Tale of America’s Opiate Epidemic. New York, NY: Bloomsbury Press; 2015.
6. National Center for Health Statistics. Drug overdose deaths in the United States, 2001–2021. NCHS Data Brief No. 457. Centers for Disease Control and Prevention website. December 2022. https://www.cdc.gov/nchs/products/databriefs/db457.htm. Accessed May 28, 2026.
7. National Center for Health Statistics. Drug overdose deaths in the United States, 2002–2022. NCHS Data Brief No. 491. Centers for Disease Control and Prevention website. March 2024. https://www.cdc.gov/nchs/products/databriefs/db491.htm. Accessed May 28, 2026.
8. National Center for Health Statistics. Drug overdose deaths in the United States, 2003–2023. NCHS Data Brief No. 522. Centers for Disease Control and Prevention website. December 2024. https://www.cdc.gov/nchs/products/databriefs/db522.htm. Accessed May 28, 2026.
9. National Center for Health Statistics. Drug overdose deaths in the United States, 2023–2024. NCHS Data Brief No. 549. Centers for Disease Control and Prevention website. January 2026. https://www.cdc.gov/nchs/products/databriefs/db549.htm. Accessed May 28, 2026.
10. National Center for Health Statistics. Provisional drug overdose death counts. Centers for Disease Control and Prevention website. Reviewed May 13, 2026. https://www.cdc.gov/nchs/nvss/vsrr/drug-overdose-data.htm. Accessed May 28, 2026.
11. Van Zee A. The promotion and marketing of oxycontin: commercial triumph, public health tragedy. Am J Public Health. 2009;99(2):221-227.
12. Carrasco-Labra A, Polk DE, Urquhart O, et al. Evidence-based clinical practice guideline for the pharmacologic management of acute dental pain in adolescents, adults, and older adults: a report from the American Dental Association Science and Research Institute, the University of Pittsburgh, and the University of Pennsylvania. J Am Dent Assoc. 2024;155(2):102-117.e9.
13. Brunton L, Chabner B, Knollman B, eds. Goodman and Gilman’s The Pharmacological Basis of Therapeutics. 12th ed. McGraw-Hill Education; 2011.
14. Theken KN, Chen M, Wall DL, et al. A randomized, double-blind pilot study of analgesic and anti-inflammatory effects of naproxen sodium and acetaminophen following dental implant placement surgery. Front Pharmacol. 2023;14:1199580.
15. Dionne RA, Gordon SM, Moore PA. Prescribing opioid analgesics for acute dental pain: time to change clinical practices in response to evidence and misperceptions. Compend Contin Educ Dent. 2016;37(6):372-378.
16. Gordon SM, Brahim JS, Dubner R, et al. Attenuation of pain in a randomized trial by suppression of peripheral nociceptive activity in the immediate postoperative period. Anesth Analg. 2002;95(5):1351-1357.
Figures and Images
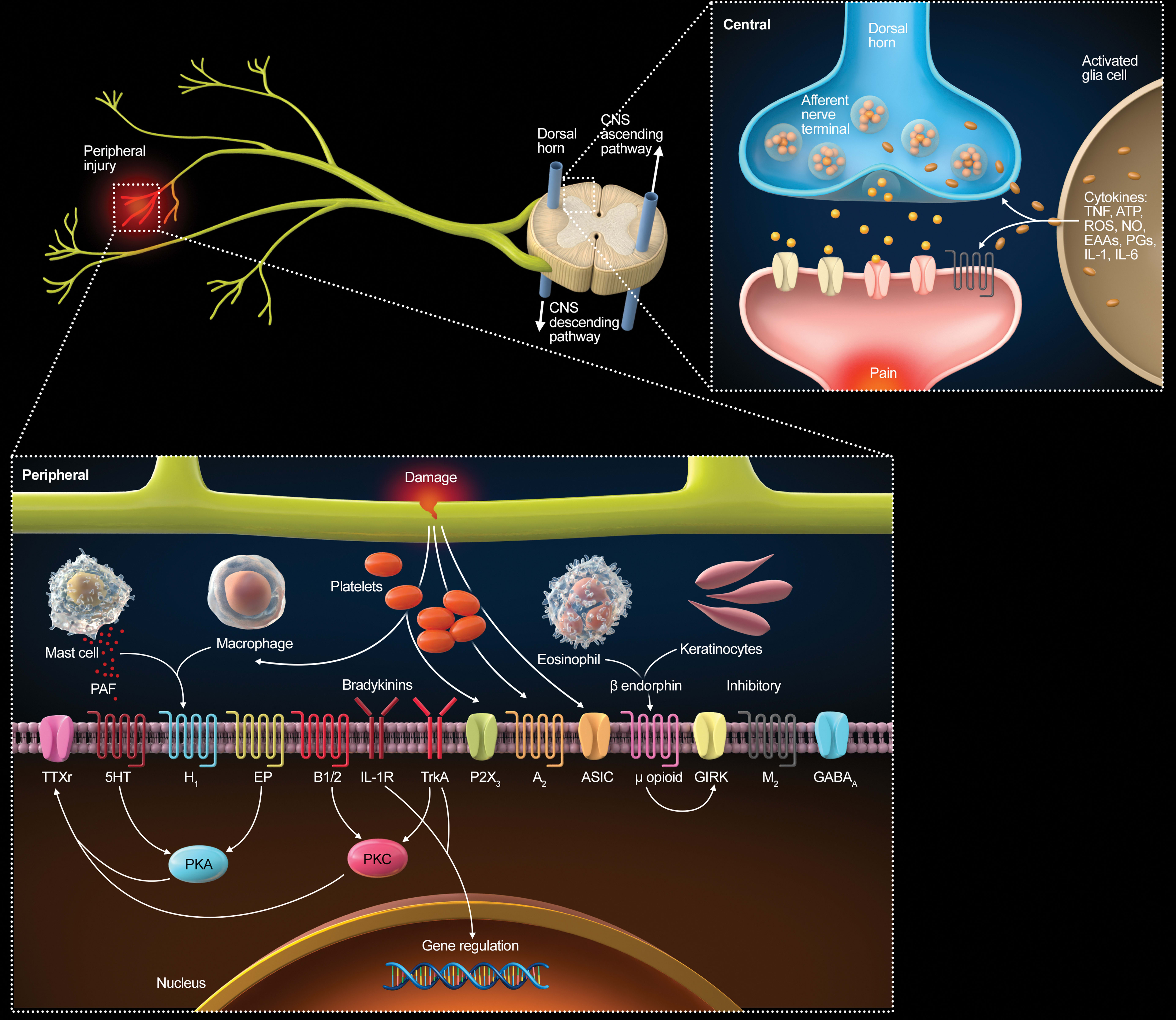
Figure 1
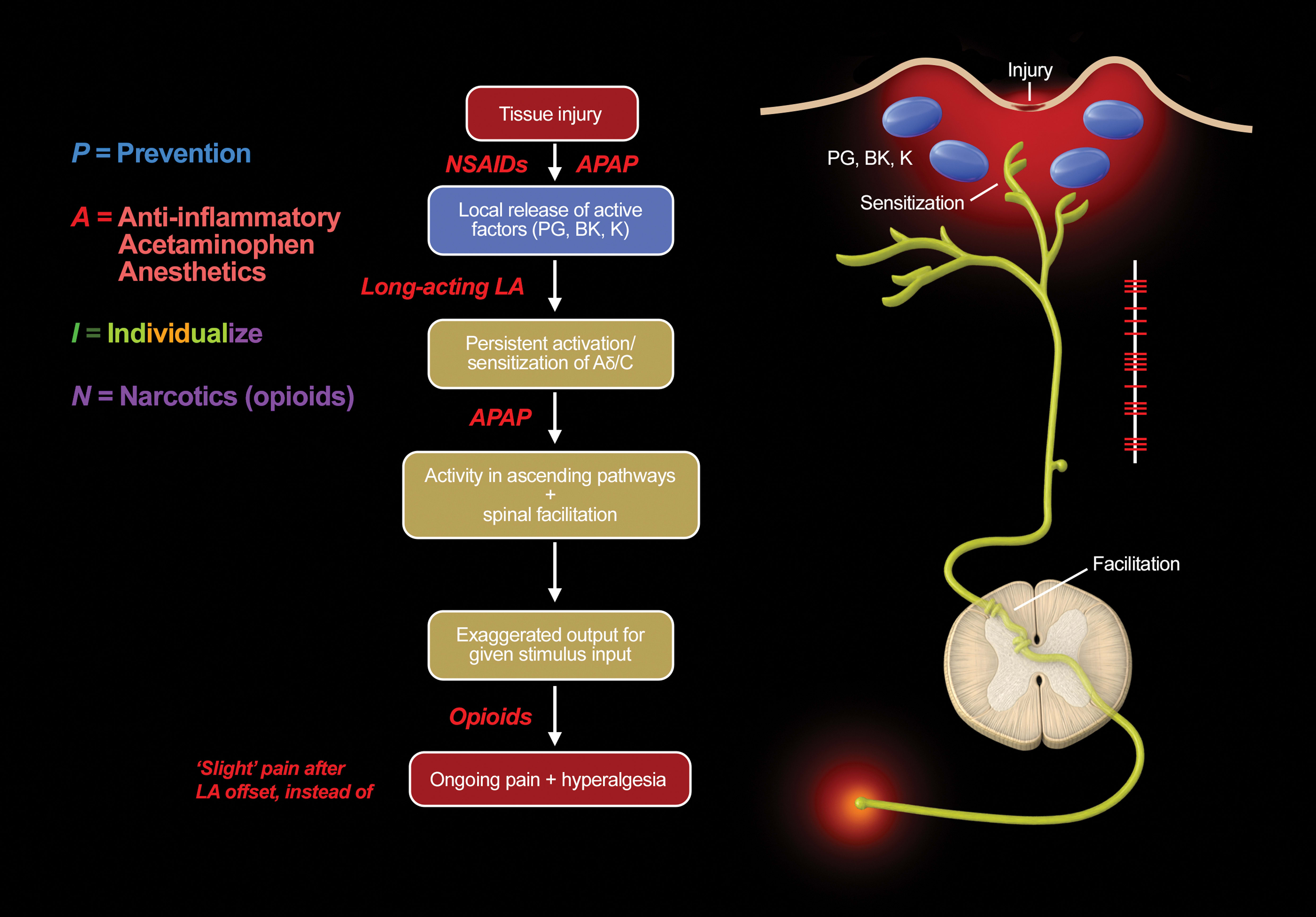
Figure 2
