Abstract: Background: Alveolar ridge deficiencies following trauma, tooth loss, or endodontic pathology may compromise implant placement in the anterior maxilla. While autogenous bone grafting remains the benchmark, a growth factor bioavailability–enhanced allograft (GFBA) has been developed as an alternative. Case Presentation: A 44-year-old man presented for implant rehabilitation in the anterior maxilla. Tooth No. 8 was missing due to trauma that occurred approximately 20 years prior. Cone-beam computed tomography findings for site No. 8 showed an atrophic alveolar ridge with intact cortical plates and no intraosseous pathology, but insufficient ridge volume. Tooth No. 7 had been previously endodontically treated and exhibited periapical rarefying osteitis, buccal cortical plate dehiscence, and widening of the periodontal ligament space, consistent with a persistent inflammatory process. Treatment involved extraction of tooth No. 7 with socket debridement and grafting using a GFBA and ridge augmentation at site No. 8 using an autogenous ramus block graft. Results: At 11 months, both sites demonstrated successful ridge augmentation. The GFBA site showed a homogeneous trabecular pattern and advanced integration, while the autogenous graft demonstrated ongoing remodeling and graft integration. Implants were placed successfully at both sites, with follow-up radiographs confirming stable peri-implant bone levels and successful osseointegration. Conclusion: GFBA may serve as an alternative to autogenous bone grafting in moderate ridge defects.
Alveolar ridge preservation and augmentation are essential in implant dentistry to allow for placement of implants in prosthetically ideal positions. Following tooth extraction, significant dimensional changes can occur, including reductions in ridge width and height, particularly within the first 1 to 3 years. These changes may be exacerbated by traumatic injury or pre-existing endodontic or periodontal pathology, often necessitating ridge augmentation to achieve optimal esthetic and functional outcomes.1,2
While autogenous bone grafting remains the gold standard approach for alveolar ridge augmentation,3 it is associated with donor site morbidity and increased surgical complexity.4 Traditional bone graft substitutes such as xenografts and mineralized allografts provide osteoconductive scaffolding but lack biological signaling, limiting their suitability for regeneration of large defects or in compromised patients.5 Demineralized allografts contain growth factors that can enhance their regenerative potential6; however, the amount of these growth factors varies significantly between donors,7,8 and their potential benefit is reduced by limited release of growth factors from the matrix.9,10 A growth factor bioavailability–enhanced allograft (GFBA) bone graft substitute has been introduced that claims to have enhanced osteoinductive potential due to increased release of endogenous growth factors, including bone morphogenetic proteins (BMPs), from the allograft matrix.11 Clinically, GFBA has been reported to have similar outcomes to autogenous bone graft when used in lumbar spine fusions.12

S Series Implant Portfolio
This case report presents a direct intrapatient comparison of GFBA and autogenous bone when used to restore the maxillary alveolar ridge and in determining whether the augmented ridge supports dental implant placement. The case report was approved by Veritas Central Institutional Review Board and included a subject consent waiver (2026-3932-24089-4).
Case Presentation
Preoperative Condition
A 44-year-old male patient presented to the author’s clinic for implant consultation regarding tooth No. 8. His medical history was significant for asthma (last episode approximately 15 years prior) and he reported social use of alcohol and cannabis. The patient sustained dental trauma on two separate occasions approximately 20 years previously, ultimately resulting in the loss of tooth No. 8. At presentation, a fixed anterior prosthesis was in place with tooth No. 7 serving as the distal abutment; a periapical lesion associated with tooth No. 7, however, was noted (Figure 1 and Figure 2).
Clinical and radiographic examination revealed a hybrid periodontal biotype and a severe buccal concavity at site No. 8. Tooth No. 7 demonstrated features consistent with periapical rarefying osteitis. The patient exhibited a medium smile line, adequate opposing occlusion, and an alveolar ridge at site No. 8 that was inadequate for implant placement. Preoperative cone-beam computed tomography (CBCT) confirmed an atrophic ridge at site No. 8 with significant loss of buccal bone. Additionally, the periapical rarefying osteitis exhibited by tooth No. 7 extended to a buccal cortical plate dehiscence. Preoperative CBCT and periapical radiograph images are presented in Figure 3 through Figure 8.
Treatment Planning
The treatment plan consisted of: (1) extraction of tooth No. 7 with socket debridement and ridge preservation using GFBA to address the horizontal deficiency; and (2) horizontal ridge augmentation at site No. 8 utilizing an autogenous ramus block graft. The autogenous block graft was selected for site No. 8 because of the severity of the horizontal defect compared to site No. 7. Dental implants (3.3 mm x 10 mm) were planned for placement at sites Nos. 7 and 8 following an appropriate healing period.
Surgical Procedure
Under general anesthesia via nasal intubation, a crestal incision from tooth No. 7 to tooth No. 9 with vertical releases was performed, and a full-thickness mucoperiosteal flap was elevated to expose the anterior maxilla. Tooth No. 7 was extracted, and the associated chronic periapical lesion was curetted. The buccal wall in site No. 7 was not present following the extraction of the tooth. Ridge augmentation was performed using 2.5 cc of GFBA (Induce NMP® Fibers, Induce Biologics, inducebiologics.com), rehydrated with 2 cc of sterile saline and mixed with <0.5 cc of mineralized cortical particulate allograft. A submucosal vestibuloplasty was completed to facilitate tension-free closure.
Autogenous bone was harvested from the right mandibular ramus via a crestal incision with distal release in the region of tooth No. 31. A lateral ramus osteotomy was performed using a #701 bur under copious irrigation, and a cortical block graft was obtained.
The recipient site No. 8 (~10 mm x 9 mm) was prepared with a bony shelf to allow passive adaptation of the graft. The block graft was contoured and secured with a 1.5 mm x 9 mm fixation screw. Additional mineralized cortical particulate allograft was applied.
Guided bone regeneration was performed using a resorbable, type I bovine collagen membrane (30 mm x 40 mm), and primary closure was achieved.
Grafing Results and Implant Placement
Healing was uneventful and there were no adverse reactions associated with use of the GFBA graft. Eleven months after grafting, the sites were imaged using CBCT (Figure 9 through Figure 11). The GFBA grafted site showed trabeculated mineralized tissue throughout the grafted area that appeared to be well integrated into the alveolar bone (Figure 9 and Figure 11). Imaging of the autogenous bone graft showed that it maintained its density (Figure 10 and Figure 11).
Dental implants (Straumann Bone Level Tapered™, 3.3 mm x 10 mm, Straumann, straumann.com) were successfully placed at sites Nos. 7 and 8 without the need for additional grafting (Figure 12).
At 5 months post–implant placement both implants were found to be stable, with CBCT and radiography showing that the sites had maintained crestal bone levels, and there was no peri-implant radiolucency (Figure 13 and Figure 14).
Clinical and radiographic images of the final prostheses are shown in Figure 15 through Figure 18.
Discussion
Reconstruction of alveolar ridge deficiencies in the anterior maxilla requires careful selection of grafting materials and techniques to achieve both functional implant support and optimal esthetic outcomes. The decision to use an autogenous block graft at site No. 8 and GFBA at site No. 7 was guided by the extent of the defects, the need for structural stability, and the biological requirements for predictable bone regeneration.
In cases of moderate to severe ridge deficiency, particularly when 3-dimensional reconstruction is required, block grafts harvested from intraoral sites such as the mandibular ramus provide immediate structural support and facilitate restoration of ridge contour.13 Additionally, rigid fixation of the block graft allows for revascularization and graft incorporation—critical for long-term stability and successful implant placement. Studies have demonstrated high predictability of horizontal ridge augmentation using autogenous block grafts, particularly in the anterior maxilla where esthetic demands are high and bone volume is often limited.13,14
The use of autogenous grafts alone, however, is associated with limitations that include donor site morbidity, limited graft volume, and increased surgical time. To mitigate these challenges and optimize graft handling and contouring, particulate graft materials are frequently used. Mineralized bone allograft such as freeze-dried bone allograft (FDBA) provides an osteoconductive scaffold that facilitates bone formation while reducing the need for additional autogenous bone harvesting. The use of FDBA has been shown to support new bone formation and contribute to volume maintenance when used in ridge augmentation procedures; however, the slow resorption of the FDBA particles results in a lower amount of vital bone in the graft site than in ungrafted sites.15,16 In contrast, demineralized FDBA (DFDBA) is more rapidly resorbed and does not impede new bone formation at the graft site.16 Further, with demineralization, BMPs that are present within the collagenous matrix are able to elute out of the graft providing osteoinductive potential to the graft material.6 However, because up to 90% of the BMPs remain bound to the demineralized matrix, the osteoinductive potential of DFDBA is limited.9
Recently, a GFBA has become available that undergoes a novel processing method to increase the bioavailability of the BMPs. Smith et al showed that GFBA had increased osteoinductive potential in vitro and in vivo compared to DFDBA,11 while a clinical study evaluating GFBA in 50 patients undergoing anterior lumbar interbody fusion reported fusion rates similar to those previously reported for autogenous bone,12 suggesting GFBA may be suitable as an alternative to autogenous bone. GFBA fibers were used because they resisted graft migration and were easily molded, allowing for improved adaptation to the recipient site and enhanced contouring of the augmented ridge.
Because the GFBA is initially radiolucent11 the appearance of mineralized tissue within the grafted volume represents regeneration of new bone. In contrast, the block autogenous grafted in the present case appeared dense indicating that the grafted region comprised the original grafted cortical bone that was still undergoing remodeling and integration with the residual alveolar bone, which is typical for block autogenous grafts.3
Both grafting approaches achieved sufficient bone for implant placement, and imaging of the sites 5 months post–implant placement showed there was no peri-implant radiolucency, which is consistent with successful osseointegration. These findings support a defect-based approach, where GFBA can be considered a less invasive alternative to autogenous bone grafts for moderate defects.
Conclusion
GFBA can provide predictable ridge augmentation. In this comparative evaluation, GFBA and autogenous bone grafting both resulted in successful implant outcomes. GFBA represents a clinically effective and less invasive alternative in appropriate cases, supporting its consideration for use in moderate ridge deficiencies.
DISCLOSURE
The author has no disclosures to report but is in talks regarding a potential future partnership with Induce Biologics.
About the Author
Ren Chang, DDS
Private Practice in Oral and Maxillofacial Surgery, Toronto, Ontario, Canada; Fellow, Royal College of Dentists of Canada
References
REFERENCES
1. Johnson K. A study of the dimensional changes occurring in the maxilla following tooth extraction. Aust Dent J. 1969;14(4):241-244.
2. Schropp L, Wenzel A, Kostopoulos L, Karring T. Bone healing and soft tissue contour changes following single-tooth extraction: a clinical and radiographic 12-month prospective study. Int J Periodontics Restorative Dent. 2003;23(4):313-323.
3. Misch CM. Maxillary autogenous bone grafting. Oral Maxillofac Surg Clin North Am. 2011;23(2):229-238.
4. Caldwell S. Bone grafting complications. In: Misch CE, Resnik RR, eds. Misch’s Avoiding Complications in Oral Implantology. Mosby; 2018:440-498.
5. Chan M. Bone-grafting techniques and biomaterials for alveolar ridge augmentation. In: Dym H, Halpern LR, Ogle OE, eds. Oral and Maxillofacial Surgery, Medicine, and Pathology for the Clinician. John Wiley & Sons, Inc.; 2023:45-83.
6. Gruskin E, Doll BA, Futrell FW, et al. Demineralized bone matrix in bone repair: history and use. Adv Drug Deliv Rev. 2012;64(12):1063-1077.
7. Pietrzak WS, Woodell-May J, McDonald N. Assay of bone morphogenetic protein-2, -4, and -7 in human demineralized bone matrix. J Craniofac Surg. 2006;17(1):84-90.
8. Murray SS, Brochmann EJ, Harker JO, et al., A statistical model to allow the phasing out of the animal testing of demineralised bone matrix products. Altern Lab Anim. 2007;35(4):405-409.
9. Pietrzak WS, Dow M, Gomez J, et al. The in vitro elution of BMP-7 from demineralized bone matrix. Cell Tissue Bank. 2012;13(4):653-661.
10. Pietrzak WS, Ali SN. The elution kinetics of BMP-2, BMP-4, and BMP-7 from a commercial human demineralized bone matrix putty. J Craniofac Surg. 2017;28(8):2183-2188.
11. Smith MR, Shivanna S, Kohen Y, et al. Development of a growth factor bioavailability enhanced allograft (GFBA) for bone regeneration. Cell Tissue Bank. 2026;27(1):6.
12. Nunley PD, Tran S, Stone M. Clinical evaluation of a growth factor bioavailability enhanced allograft in anterior lumbar interbody fusion (ALIF). J Spine Surg. 2025;11(4):840-850.
13. Khoury F, Hanser T. Mandibular bone block harvesting from the retromolar region: a 10-year prospective clinical study. Int J Oral Maxillofac Implants. 2015;30(3):688-697.
14. Cordaro L, Amadè DS, Cordaro M. Clinical results of alveolar ridge augmentation with mandibular block bone grafts in partially edentulous patients prior to implant placement. Clin Oral Implants Res. 2002;13(1):103-111.
15. Iasella JM, Greenwell H, Miller RL, et al. Ridge preservation with freeze-dried bone allograft and a collagen membrane compared to extraction alone for implant site development: a clinical and histologic study in humans. J Periodontol. 2003;74(7):990-999.
16. Canellas JVDS, Ritto FG, Figueredo CMDS, et al. Histomorphometric evaluation of different grafting materials used for alveolar ridge preservation: a systematic review and network meta-analysis. Int J Oral Maxillofac Surg. 2020;49(6):797-810.
Figures and Images

Figure 1

Figure 2
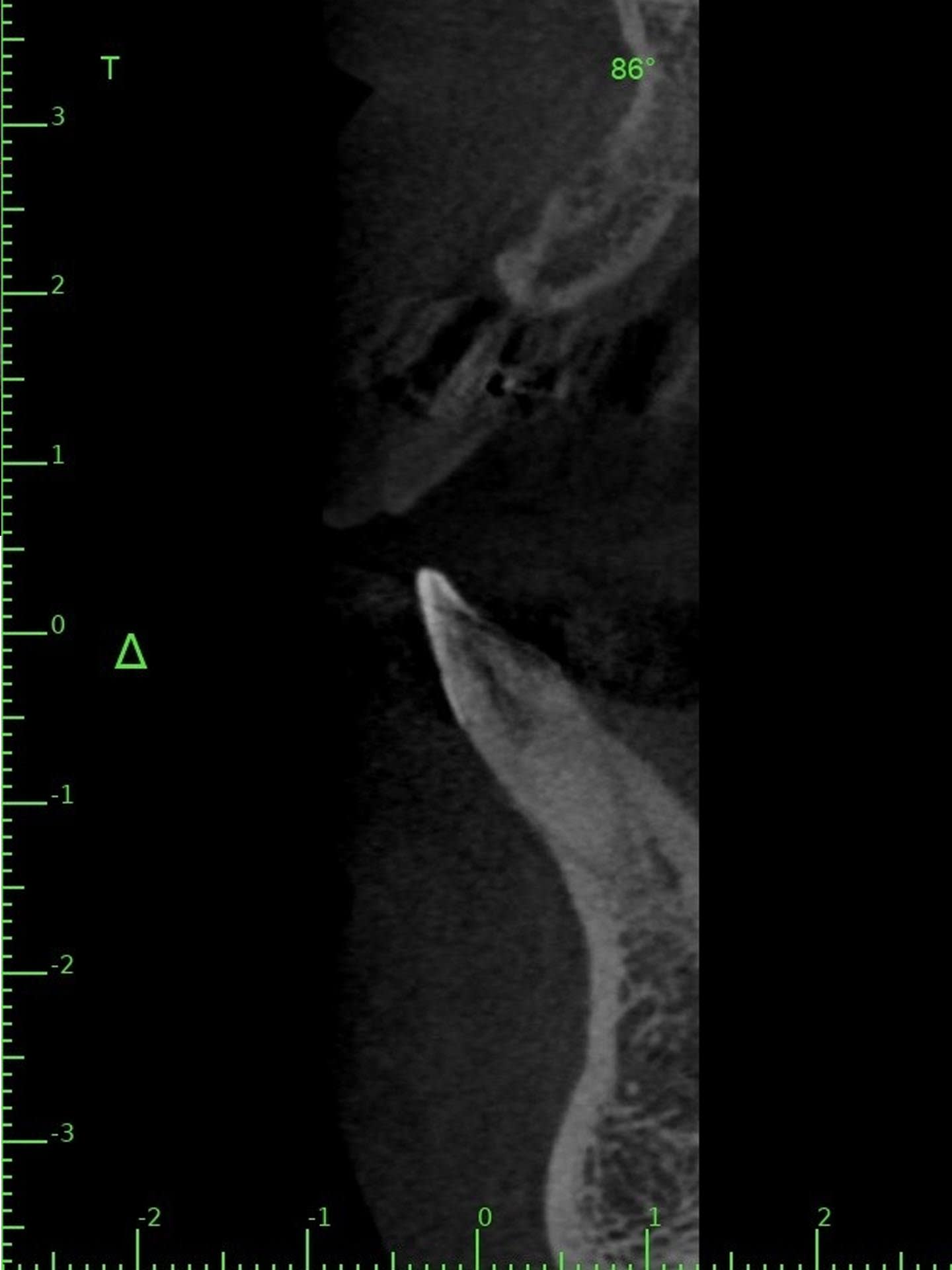
Figure 3

Figure 4
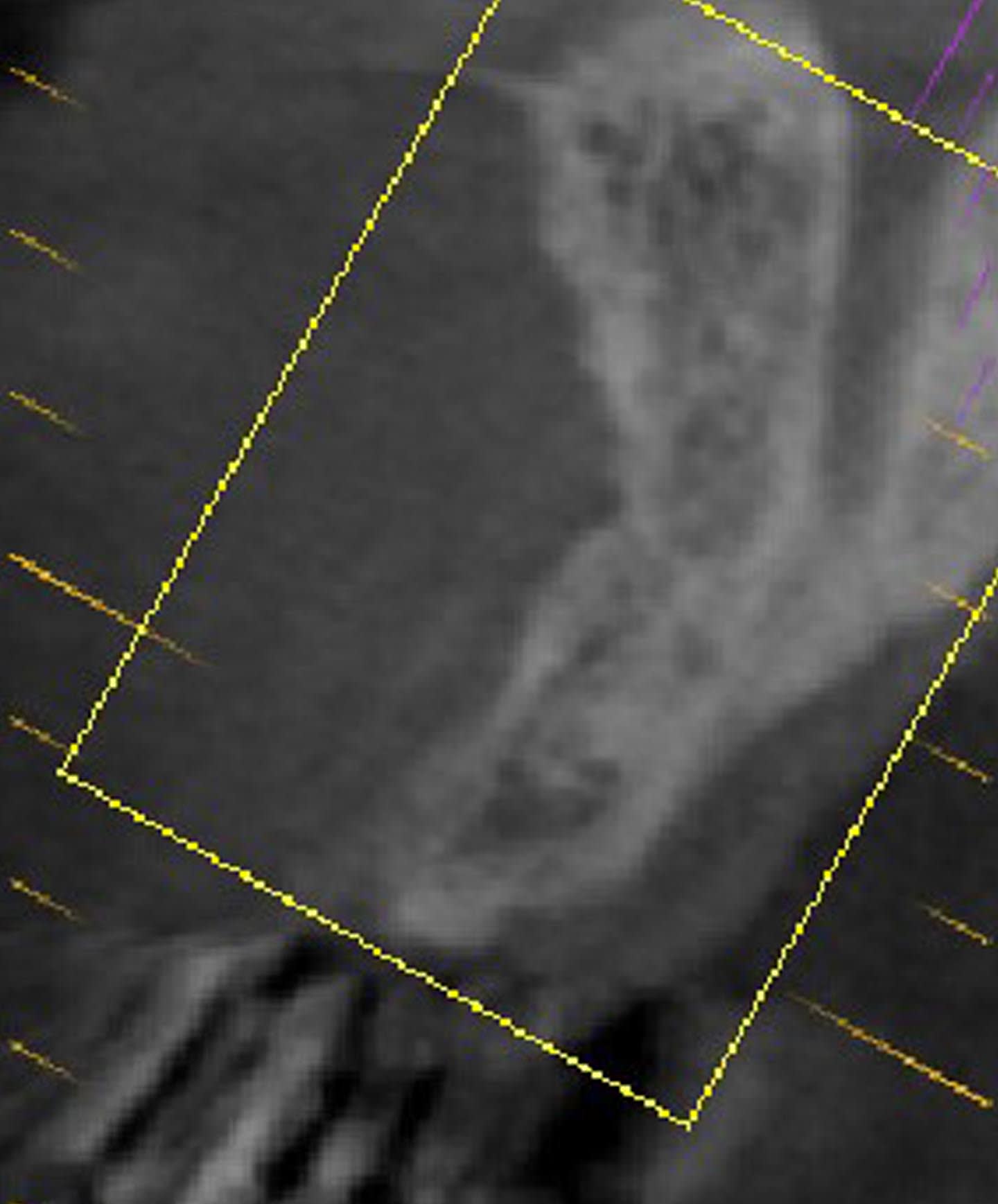
Figure 5
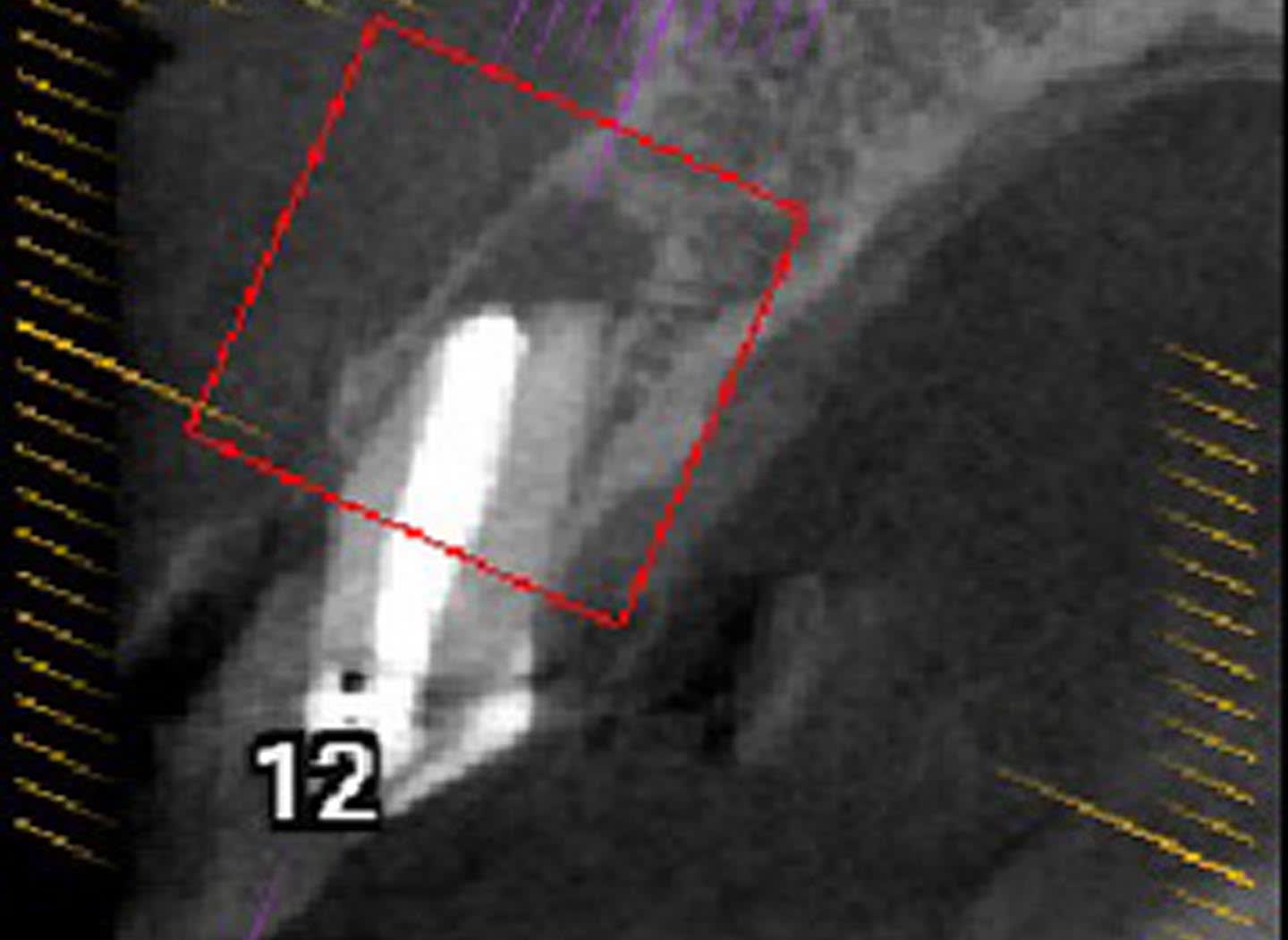
Figure 6

Figure 7
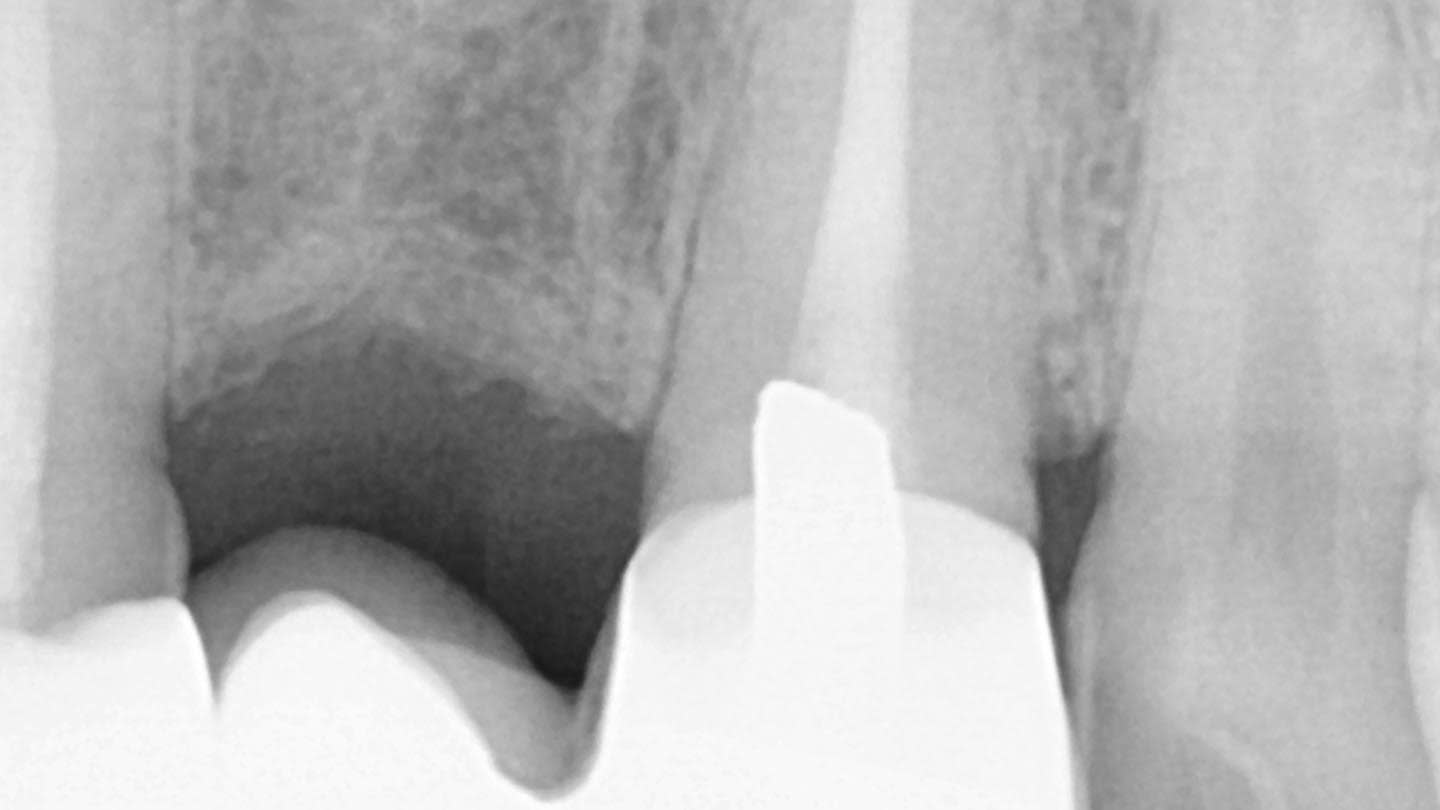
Figure 8

Figure 9

Figure 10
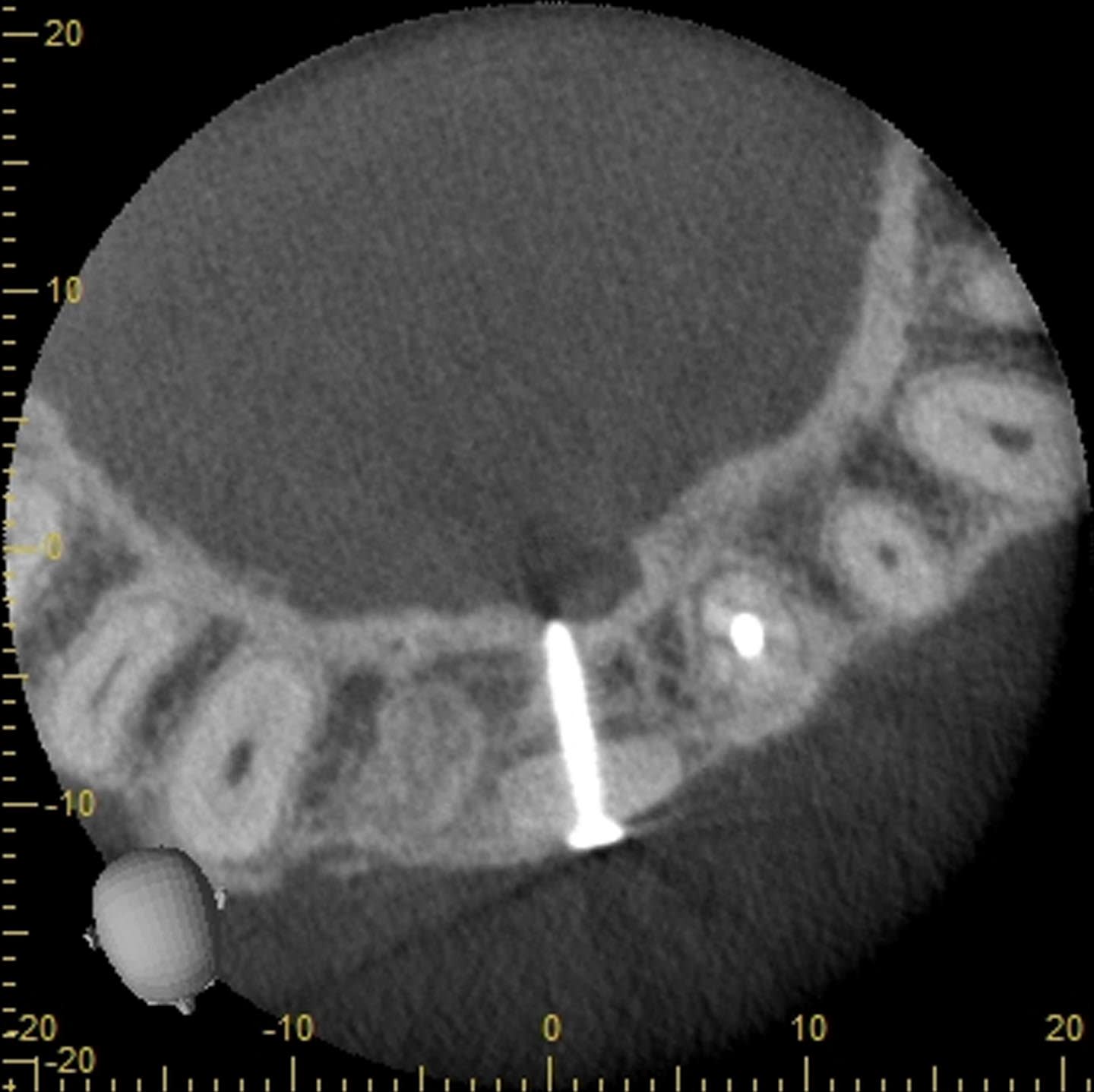
Figure 11
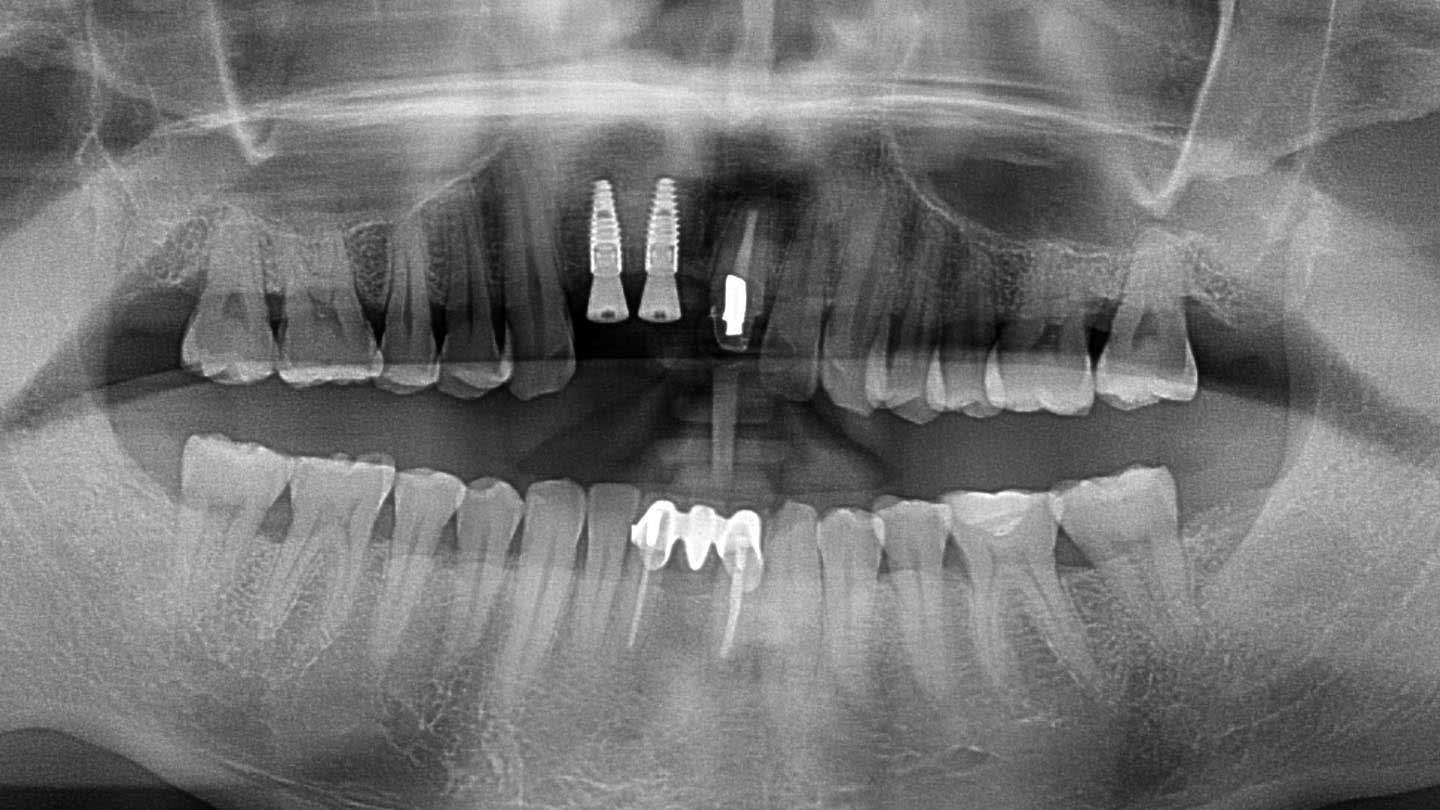
Figure 12
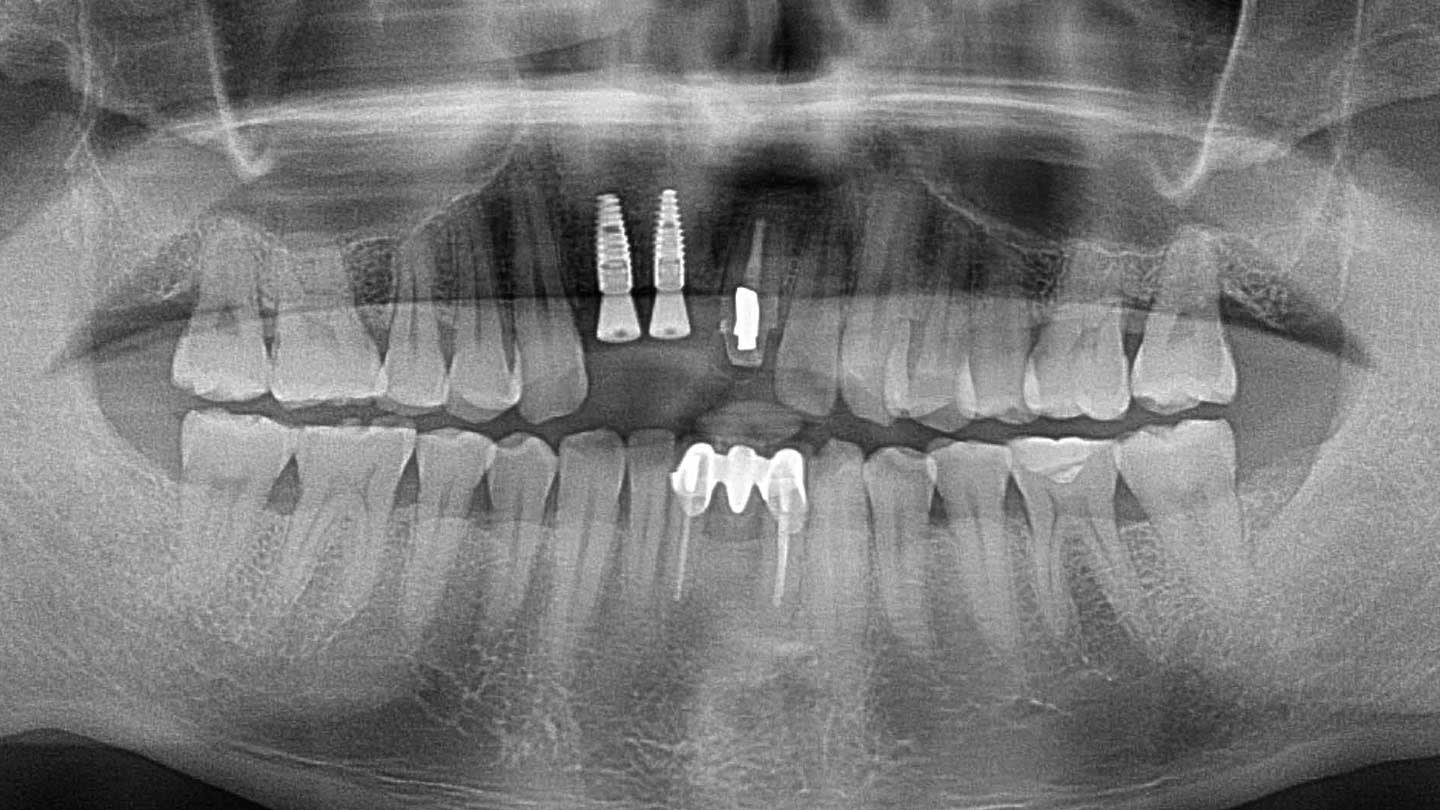
Figure 13

Figure 14

Figure 15

Figure 16

Figure 17

Figure 18
