Abstract: One of the toughest challenges in esthetic dentistry is to match the shade of full-coverage crowns and resin-bonded laminate veneers on maxillary incisors. This is particularly difficult when dealing with dissimilar underlying substrates, varying levels of tooth discoloration, and different amounts of sound structure. This clinical report describes an alternative approach for matching the color shade in the anterior area to overcome substrate-related esthetic limitations. To facilitate the tooth being crowned, a core was made from high-opacity lithium-disilicate ceramic, with the shape and shade of the adjacent teeth prepared for veneers. Four veneers were fabricated from high-translucency lithium-disilicate ceramic and bonded to the natural teeth and the lithium-disilicate core using the same resin-based composite cement to achieve a uniform shade on all restored teeth. A digital workflow was applied to design and manufacture the restorations. This case report demonstrates that the combination of a medium- or high-opacity lithium-disilicate substructure and thin veneers, supported by a digital planning workflow, can provide a viable solution for anterior cases with varying substrate discoloration and restoration thickness.
The primary goal of esthetic dentistry is to replicate the morphology and appearance of natural teeth so that indirect dental restorations blend seamlessly with the patient’s existing dentition. Achieving a natural-looking, even shade across various types of restorations is critical to effectively match optical properties among the restorations and with adjacent natural teeth.1 This endeavor poses a significant challenge, particularly when maxillary incisors are involved.
Natural teeth vary in terms of optical parameters, including chroma, value, hue, translucency, surface texture, and other unique optical effects. Factors such as the amount of tooth preparation and reduction, material properties, luting agent shade, and ceramic thickness significantly influence the final esthetic outcome.2,3
Among the ceramic systems available on the market, heat-pressed glass-ceramic lithium-disilicate (LDS) structures have become popular due to their excellent esthetic and mechanical properties (350 MPa to 450 MPa).4,5 Although ceramic systems may be used to improve the color and translucency of the restorations, a perfect result cannot be guaranteed.6 Ceramics that are more translucent allow more light to enter and scatter, which means that the underlying tooth has a significant influence over the resultant color. Adjusting the thickness and opacity of the ceramic can help clinicians control the overall translucency of the restoration. Additionally, the color of the resin cement also impacts the final color.1,3
In cases where incisors have varying amounts of remaining tooth structure and color, for example, endodontically treated teeth, a combination of a veneer over an opaque-core crown can be a reliable solution. This approach minimizes the influence of the abutment shade on the ceramic veneer to be bonded on top of it. When the core is designed with the same shape and shade as the adjacent teeth prepared for veneers, the same veneer thickness can be applied to both the crown and the teeth, achieving a seamless blend of value and opacity.7,8
Clinical Case Report
A 40-year-old male patient presented to the author’s (MR) office with the request to improve the esthetics of his smile, as there were several extensive infiltrated composite restorations and a chipped crown showing a severe dark color on an endodontically treated tooth (Figure 1 and Figure 2).
Following a comprehensive clinical, radiographic, and initial photographic assessment, ceramic restorations were chosen to restore function and esthetics. Given that the underlying structure of tooth No. 9 was presented with a fractured crown, a metal cast post, and dark discoloration, it was decided to fabricate a crown with an opaque core using high-opacity LDS ceramic along with a bonded lithium-disilicate veneer on top to enhance the esthetic outcome. For teeth Nos. 7, 8, and 10, LDS ceramic veneers were chosen.
Digital Smile Design
Initial intraoral scans were taken, and a digital smile design protocol was performed by the author to develop a facially driven digital wax-up for the maxillary anterior teeth due to differences in tooth proportion and the deficient tooth No. 9 crown (TRIOS Smile Design, 3Shape, 3shape.com).
Consistent measurements act as a strict quality control mechanism, ensuring precision and accuracy throughout the design and treatment process.9-11 When planning esthetic restorative cases on patients with high expectations, the use of a wax-up and mock-up is essential for effective communication.12 The mock-up technique allows for a 3-dimensional (3D) visualization of the anticipated result over time, including tooth proportion, morphology, phonetics, amount of tooth reduction, and functional and esthetic analysis, making it often preferable to 2-dimensional (2D) and 3D chairside image modification software.13,14 For the present case, after the smile design was confirmed, an extra analog wax-up was performed to provide more details and to facilitate fabrication of an intraoral direct mock-up using a silicone index and a bis-acryl material, which also served as a guide for tooth preparation (Figure 3). After analyzing the mock-up and making minor esthetic adjustments, a digital impression was captured to emulate the future design of the final restorations.
Veneer preparations on teeth Nos. 7, 8, and 10 were performed according to the APT (“aesthetic pre-evaluative temporary”) protocol,13 guided by the definitive mock-up that visualizes the final shape of the teeth to be restored. The previous silicone index was also used to check the preparation depths. Upon approval from both the clinician and patient, the intraoral mock-up serves as a precise guide for shaping the tooth structure according to the planned final contours. This ensures that only minimal preparation of the tooth structure is performed, or in some cases, no preparation may be required in certain areas. Depth cutter burs were used to achieve the treatment goals while preserving as much natural tooth structure as possible.
Lithium-Disilicate Ceramics
After crown removal on tooth No. 9, recontouring, and polishing, and veneer preparations of teeth Nos. 7, 8, and 10, the patient’s upper and lower arches were digitally scanned (TRIOS 4, 3Shape). These scans, along with digital photographs, were uploaded and integrated into the software (Digital Smile System SRL, digitalsmiledesign.com) for the virtual planning of the four veneers on teeth Nos. 7 through 10 and the opaque-core crown for No. 9 (Figure 4 through Figure 6). Ceramics with medium or high opacity, intended for the fabrication of core structures, were appropriate for this case. A lithium disilicate–reinforced monochromatic ceramic block with high-opacity color for CAD/CAM technology (IPS e.max®, Ivoclar, ivoclar.com) was used to fabricate the core for tooth No. 9. Then, it was fired in an oven (Zubler Vario Press 300, Jensen Dental, jensendental.com) for 5 minutes at 750°C and for 10 minutes at 850°C to complete crystallization, according to the manufacturer’s recommendations.
The typical thickness of a ceramic crown is generally between 1.5 mm and 2 mm. In many studies, increasing the thickness and opacity of the ceramic to mask the underlying color is accompanied by better matching color results.3,15 Chaiyabutr et al found that dark-colored abutment teeth exhibited the highest color difference values compared to other configurations, and the most significant color change was attributed to the nickel-chromium (Ni-Cr) post core.1 Other studies show that the final shade of ceramic restorations can be influenced by resin cements and their optical properties.3
The opaque-core crown was tried-in on tooth No. 9 and approved in terms of marginal fit, preparation adaptation, and shade matching with the adjacent incisors. After this assessment, the crown was prepared, similar to the remaining teeth, to receive a ceramic veneer. A new digital intraoral final impression (TRIOS 4) was made for all four maxillary incisors, and the standard tessellation language (STL) files were sent to the laboratory for the manufacture of lithium-disilicate porcelain veneers (IPS e.max) using subtractive milling technology (PrograMill® PM5, Ivoclar). All data transfer from 3D planning to the laboratory CAD/CAM process is faster, easier, and more predictable than conventional methods, resulting in less manufacturing time and chairtime and enhanced final esthetic results (Figure 7 and Figure 8).16-18
Final Restorations
Rubber dam was used when bonding the final restorations. The veneer corresponding to tooth No. 9 was initially bonded to the opaque-core crown extraorally following standard protocol for silica-based ceramics,19 which included 9% hydrofluoric acid-etching (Porcelain Etch, Ultradent, ultradent.com), silane application (Monobond Plus®, Ivoclar), and application of a light-curing resin cement (Variolink® Esthetic LC, neutral shade, Ivoclar) (Figure 9 through Figure 13).
Next, the combined restoration was inserted into tooth No. 9 intraorally using a self-curing resin cement (Multilink Automix®, opaque white, Ivoclar) according to the manufacturer’s instructions. The try-in paste was always used prior to cementation to help predict the influence of the resin cement shade on the definitive restorations. For this case, white opaque cement exhibited good masking ability, especially in the cervical area. The remaining veneers were bonded with the same light-curing resin cement used in the initial bonding stage for tooth No. 9. A neutral shade was used to avoid influencing the final color of the restorations (Figure 14 through Figure 17).
After the luting procedure was completed, a water-based gel was applied to the margins of the restorations to eliminate the oxygen-inhibited layer, and then light-curing was performed for 60 seconds on each veneer. Centric and eccentric contacts were verified using articulating paper. The final results demonstrated the integration of the restorations with natural texture and morphology and an accurate shade matching (Figure 18 and Figure 19). Based on the authors’ experience, these procedures are best performed under magnification.
Discussion
This case report describes a workflow designed to enhance a patient’s smile by matching shade colors effectively when different amounts of remaining tooth structure and discolored teeth are present.
The optical behavior of all-ceramic restorations is influenced by three main factors: the underlying abutment substrate, the resin luting agent, and the intrinsic structural properties of the ceramic itself. Lithium disilicate is a ceramic material consisting of lithium disilicate and lithium orthophosphate embedded in a glass phase. The precise shape, size, and density of these crystals contribute to a restoration that exhibits high flexural strength and improved fracture resistance. Its low refractive index allows for the display of outstanding optical properties, featuring natural translucency and color stability.7,19
One primary concern regarding the use of lithium-disilicate ceramic for anterior restorations is achieving an optimal shade match, particularly in cases involving endodontically treated teeth, pre-existing metallic cast posts, or titanium implant abutments, which could result in color mismatch and shadowing of the restoration. Studies have shown that critical factors like controlling the thickness and opacity of the ceramic benefit the restoration’s overall translucency. In contrast, the choice of cement color has relatively less impact on the final esthetic outcome.3,6
A reliable approach in these scenarios is to use a crown with a more opaque core, which is minimally influenced by the color of the substrate and serves as a foundation for layering a ceramic veneer. In the present case, lithium disilicate (IPS e.max) was the ceramic of choice because it outperforms zirconia in terms of shade reproduction, according to several studies.15,20,21 Combining a medium-opacity or high-opacity crown core with a high-translucency bonded ceramic veneer on top creates an outcome that enables effective masking of a discolored substrate while delivering a predictable, esthetically pleasing result, and when adhesive cementation is performed between ceramics of identical composition, the highest bond strength values and superior long-term predictability can be achieved.3,7
Conclusion
The restorations provided in this case report successfully met the patient’s expectations, reflecting the advanced capabilities of using LDS in a tailored manner to deliver superior results. The performance of this ceramic material suggests that it is a viable option in challenging anterior cases, offering good color-matching results, excellent precision, and customization. Current limitations concerning LDS translucency should be acknowledged, as it continues to present challenges. The use of lithium-disilicate ceramic should be approached with caution, especially in clinical situations where there is significant underlying substrate discoloration. In such cases, using medium-opacity or high-opacity ceramics for core structures might be preferable, and it is recommended that the core structure be veneered with a veneering ceramic to improve esthetic outcomes.
ABOUT THE AUTHORS
Macarena Rivera, DMD, MSc
Assistant Professor, Department of Prosthodontics, University of Chile, Santiago, Chile; Adjunct Professor, Department of Preventive and Restorative Sciences, University of Pennsylvania School of Dental Medicine, Philadelphia, Pennsylvania; Private Practice, Santiago, Chile
Markus B. Blatz, DMD, PhD
Professor of Restorative Dentistry, Chair, Department of Preventive and Restorative Sciences, and Assistant Dean, Digital Innovation and Professional Development, University of Pennsylvania, School of Dental Medicine, Philadelphia, Pennsylvania
References
1. Chaiyabutr Y, Kois JC, Lebeau D, Nunokawa G. Effect of abutment tooth color, cement color, and ceramic thickness on the resulting optical color of a CAD/CAM glass-ceramic lithium disilicate–reinforced crown. J Prosthet Dent. 2011;105(2):83-90.
2. Shirani M, Emami M, Mosharraf R, et al. Comparing the color match of monolithic CAD-CAM dental ceramics with the VITA Classical shade guide. J Prosthet Dent. 2024;132(3):605-611.
3. Carrabba M, Vichi A, Tozzi G, et al. Cement opacity and color as influencing factors on the final shade of metal-free ceramic restorations. J Esthet Restor Dent. 2022;34(2):423-429.
4. van Erp AL, van der Winden E, Molenaar MC, et al. Bilayered ceramic anterior restorations with reinforcement of the incisal edge by using lithium disilicate: a multicenter retrospective survival analysis with a maximum of 6-year follow-up. J Prosthet Dent. 2023;129(5):718-724.
5. Barizon KT, Bergeron C, Vargas MA, et al. Ceramic materials for porcelain veneers: part II. Effect of material, shade, and thickness on translucency. J Prosthet Dent. 2014;112(4):864-870.
6. Czigola A, Abram E, Kovacs ZI, et al. Effects of substrate, ceramic thickness, translucency, and cement shade on the color of CAD/CAM lithium-disilicate crowns. J Esthet Restor Dent. 2019;31(5):457-464.
7. Thilagar P, Sampathkumar J, Krishnan CS, et al. Comparative evaluation of the masking ability of lithium disilicate ceramic with different core thickness on the shade match of indirect restorations over metallic substrate: an in vitro study. Contemp Clin Dent. 2019;10(1):56-63.
8. Pala K, Bindl A, Mühlemann S, et al. The capacity to change the lightness of discolored tooth substrates by means of minimally invasive restorations: perception by dentists, dental technicians, and laypersons. Int J Prosthodont. 2023;36(1):7-12.
9. Georg R. Digital smile design: utilizing novel technologies for ultimate esthetics. Compend Contin Educ Dent. 2023;44(10):567-572.
10. Silva BP, Mahn E, Stanley K, Coachman C. The facial flow concept: an organic orofacial analysis – the vertical component. J Prosthet Dent. 2019;121(2):189-194.
11. Ahmed WM, Azhari AA, Sedayo L, et al. Mapping the landscape of the digital workflow of esthetic veneers from design to cementation: a systematic review. Dent J (Basel). 2024;12(2):28.
12. Jurado CA, Villalobos-Tinoco J, Mekled S, et al. Printed digital wax-up model as a blueprint for layered pressed-ceramic laminate veneers: technique description and case report. Oper Dent. 2023;48(6):618-626.
13. Gurel G, Morimoto S, Calamita MA, et al. Clinical performance of porcelain laminate veneers: outcomes of the aesthetic pre-evaluative temporary (APT) technique. Int J Periodontics Restorative Dent. 2012;32(6):625-635.
14. Reshad M, Cascione D, Magne P. Diagnostic mock-ups as an objective tool for predictable outcomes with porcelain laminate veneers in esthetically demanding patients: a clinical report. J Prosthet Dent. 2008;99(5):333-339.
15. Skyllouriotis AL, Yamamoto HL, Nathanson D. Masking properties of ceramics for veneer restorations. J Prosthet Dent. 2017;118(4):517-523.
16. Alshali S, Asali R. Conventional and digital workflow planning for maxillary teeth restoration with porcelain laminate veneers: a clinical report. Clin Cosmet Investig Dent. 2022;14:45-53.
17. Rivera M, Blatz MB. Precision matters: the evolution of impression systems and materials. Compend Contin Educ Dent. 2024;45(3):158-159.
18. Ortensi L, Sigari G, La Rosa GRM, et al. Digital planning of composite customized veneers using Digital Smile Design: evaluation
of its accuracy and manufacturing. Clin Exp Dent Res. 2022;8(2):537-543.
19. Blatz MB, Conejo J, Alammar A, Ayub J. Current protocols for resin-bonded dental ceramics. Dent Clin North Am. 2022;66(4):603-625.
20. Al Hamad KQ, Obaidat II, Baba NZ. The effect of ceramic type and background color on shade reproducibility of all-ceramic restorations. J Prosthodont. 2020;29(6):511-517.
21. Ronaghi G, Chee W, Yeung S. Single-unit implant-supported restoration adjacent to multiple lithium disilicate restorations, an approach to an esthetic challenge: a clinical report. J Prosthet Dent. 2018;119(3):325-328.
Figures and Images

Figure 1

Figure 2

Figure 3

Figure 4
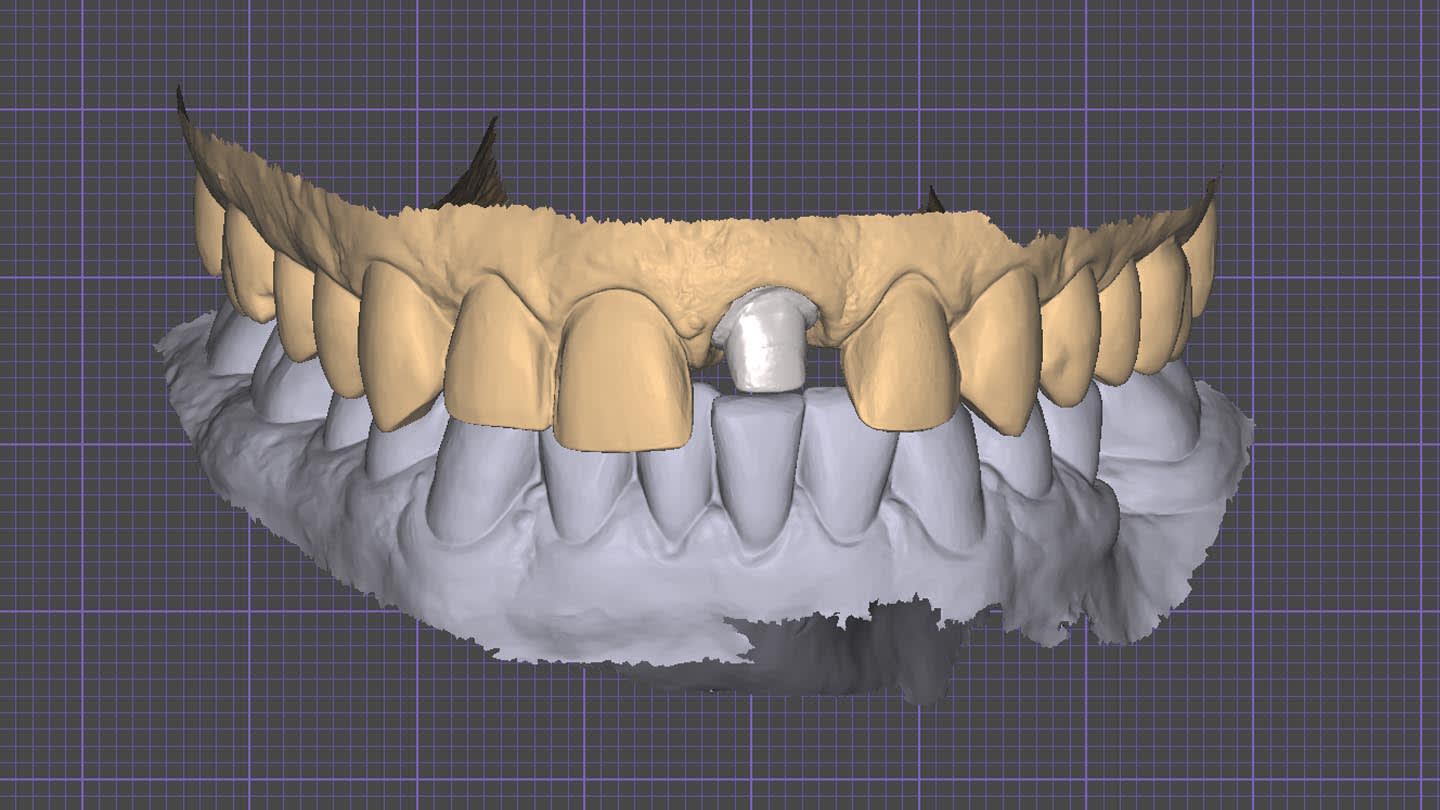
Figure 5
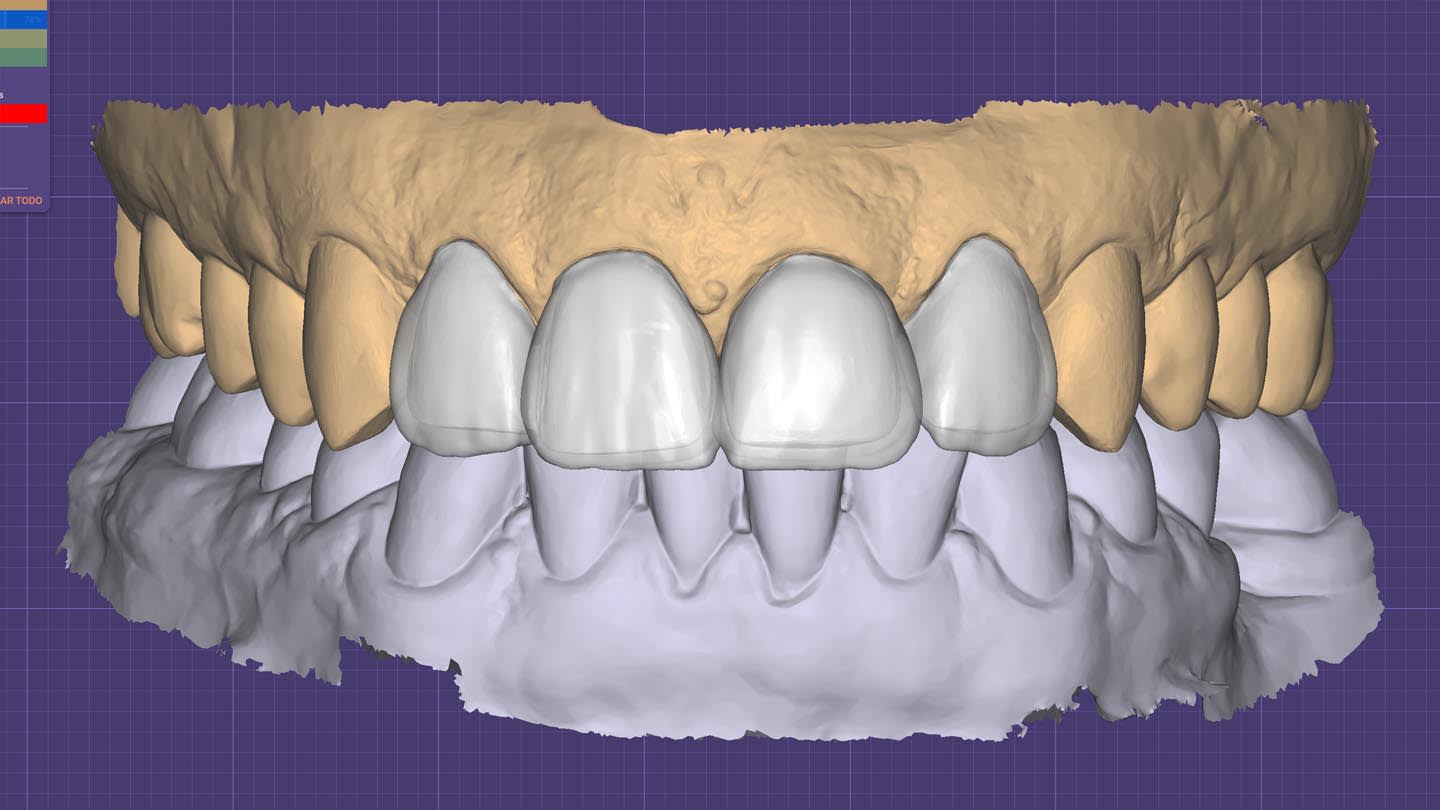
Figure 6

Figure 7
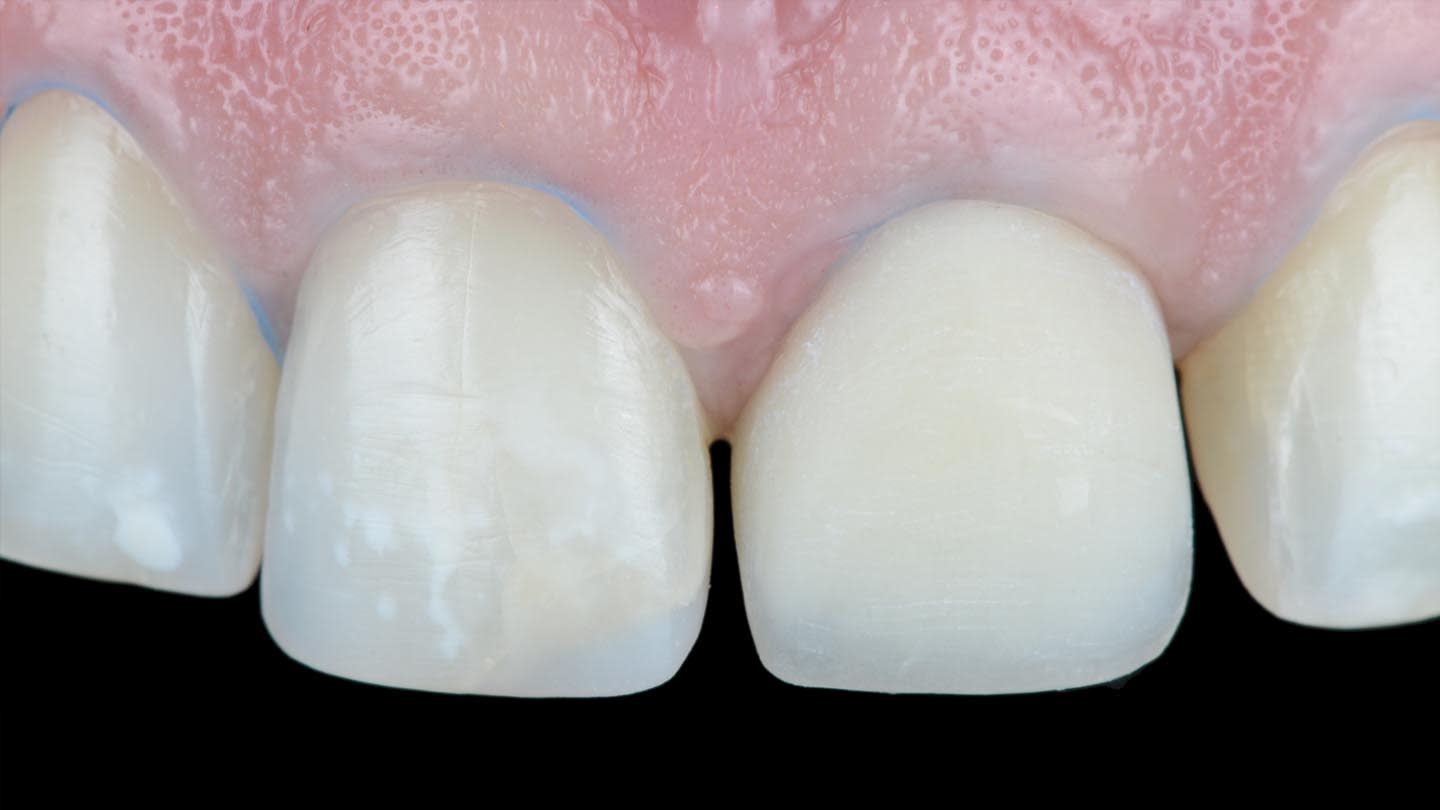
Figure 8

Figure 9

Figure 10
Figure 11

Figure 12

Figure 13

Figure 14

Figure 15
Figure 16

Figure 17

Figure 18

Figure 19