A healthy 26-year-old male patient, who had orthodontic treatment as an adolescent, was referred. During clinical assessment, class I malocclusion with moderate occlusal wear facets was observed. No mobility was present. Widened ligament spaces were noted at Nos. 14 and 15. Localized gingival inflammation was found in the maxillary left posterior sextant, with bleeding on probing. Generalized probing depths of 2–4 mm were noted, with an isolated 12 mm buccal depth on the direct buccal of No. 14 and grade 2 furcation invasion. An isolated 5–6 mm probing depth on the distal of No. 14 with grade 1 furcation invasion was also present, along with 2 mm of facial recession. Pulpal vitality testing showed normal cold response and slight percussion response, confirmed by an endodontist. The diagnosis was localized stage 3 grade B periodontitis, or severe chronic periodontitis with bruxism, trauma from occlusion, and normal pulp accompanied by symptomatic apical periodontitis. The minimally invasive, multi-step LANAP® protocol was performed using the PerioLase® MVP-7™ pulsed Nd:YAG laser (Millennium Dental Technologies, Inc., lanap.com). The patient reported minimal discomfort and returned to normal activities the following day. Radiographic imaging at 6 and 12 months post-treatment showed continual improvement in bone fill, reduced gingival inflammation, better tissue quality, and improved clinical probing depth of tooth No. 14.
KEY TAKEAWAYS
Multiple etiologies may contribute to periodontal destruction and disease progression, especially in cases with advanced furcation bone loss. Accurate diagnosis that rules out endodontic involvement is a critical component of a comprehensive assessment.
Trauma from malocclusion can exacerbate the progression of periodontal disease.
THE LASER-ASSISTED LANAP® PROTOCOL precisely targets diseased tissue while occlusal adjustment mitigates further bite trauma, resulting in true regeneration of the attachment apparatus, including new cementum, periodontal ligament, and bone. The LANAP protocol can only be performed using the PerioLase® MVP-7™ free-running pulsed Nd:YAG laser. Its variable pulse durations are particularly suited to control laser-tissue interactions.
Andrew Peterson, DMD, MS
Private Practice, Arcadia, California; Certified Instructor, Institute for Advanced Laser Dentistry
Figures and Images

Figure 1

Figure 2
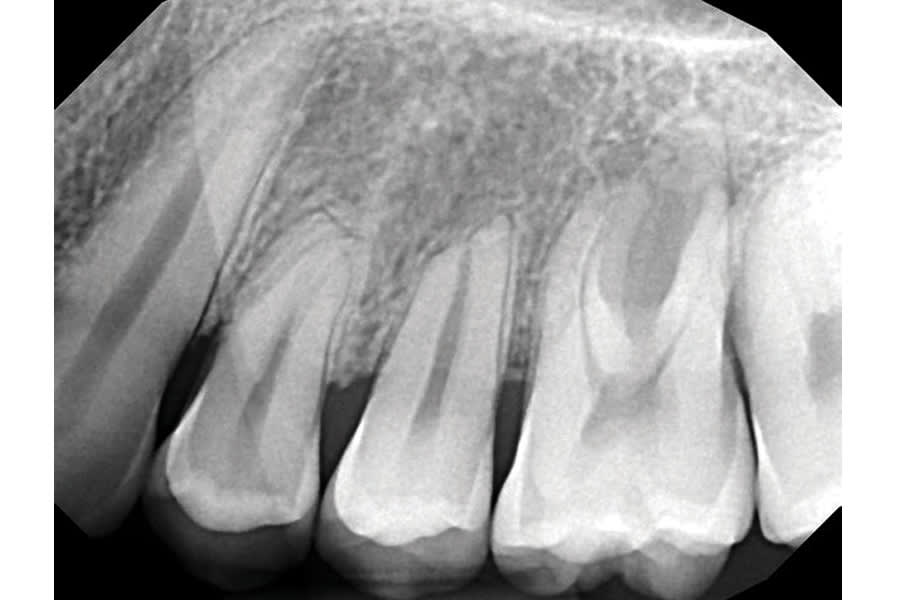
Figure 3
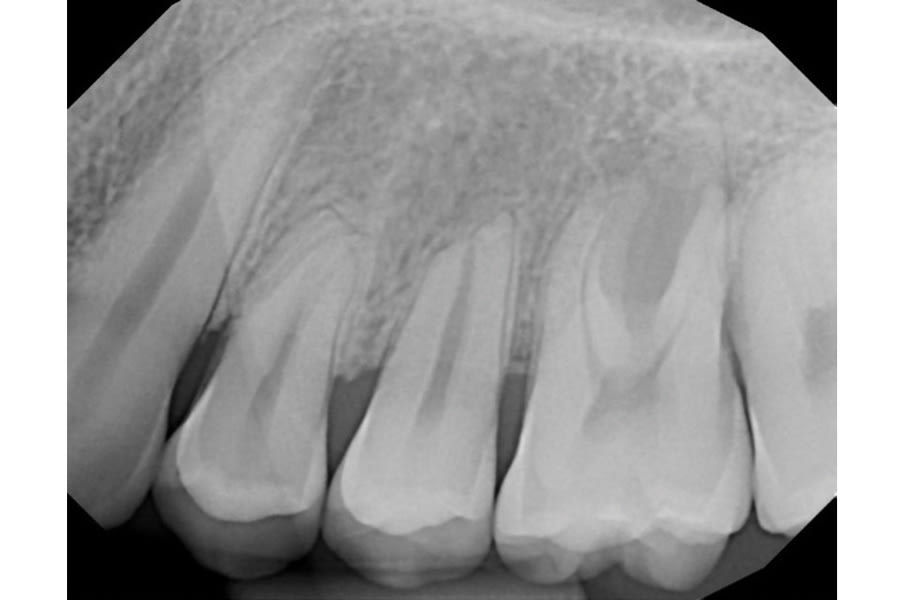
Figure 4
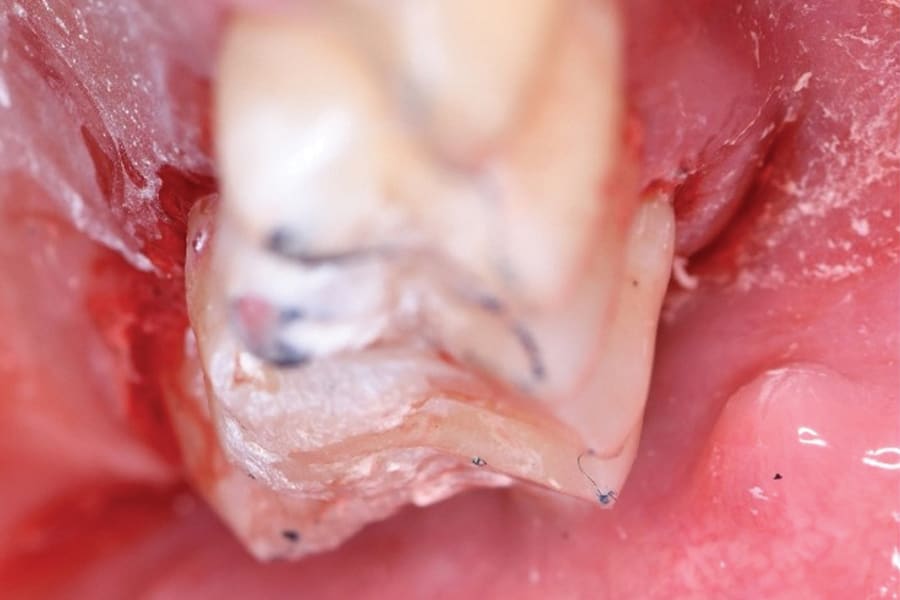
Figure 5

Figure 6
Figure 7

Figure 8
Figure 9
Figure 10
Figure 11

Figure 12

Figure 13
Figure 14
Figure 15