A 55-year-old male patient presented with advanced internal resorption of the upper right canine. The tooth was deemed nonrestorable and subsequently extracted in conjunction with alveolar ridge preservation, which was performed to attenuate post-extraction dimensional alteration. A zirconium-oxide resin-bonded fixed dental prosthesis (RBFDP) (Katana™ YML, Kuraray Noritake,
kuraraynoritake.com) was used as the long-term provisional prosthesis, bonded (CLEARFIL™ CERAMIC PRIMER PLUS, CLEARFIL™ Universal Bond Quick 2,
Panavia™ V5, Kuraray Noritake) to the first premolar. A single dental implant (BLX implant system, Straumann) was placed 4 months post-extraction in a two-stage approach with an immediate postoperative fixture-level intraoral scan done to facilitate a simultaneous implant-supported provisionalization upon fixture exposure. The provisional restoration was delivered immediately after second-stage surgery with a facial concavity to induce soft-tissue migration in the coronal direction. A conventional impression was taken, and shade information was recorded. The definitive implant-supported prosthesis was fabricated with a zirconium-oxide (Katana™ YML) framework and layered with feldspathic porcelain (Cerabien™ ZR, Kuraray Noritake) supported by a titanium base (Variobase®, Straumann). The prosthesis was designed with an emulated root form similar to the contralateral side and as appropriate for the surrounding periodontium.
KEY TAKEAWAYS
The use of modern ceramic technology allows for the fabrication of prostheses that closely replicate the appearance and function of natural teeth.
An FP2 prosthesis may serve as an alternative treatment option when soft-tissue augmentation is not indicated or pursued.
Dental photography and shade communication can help maximize clinical outcomes and aid in team collaboration.
Seung Jun Song, DMD, MS
Medical Staff, NewYork-Presbyterian Hospital, Columbia University; Assistant Professor in Dental Medicine, Columbia University, New York, New York
Sung Bin Im, MDC, CDT, BS
Chief Executive Officer, Sung Bin Im Dental Studio, Fort Lauderdale, Florida
Figures and Images
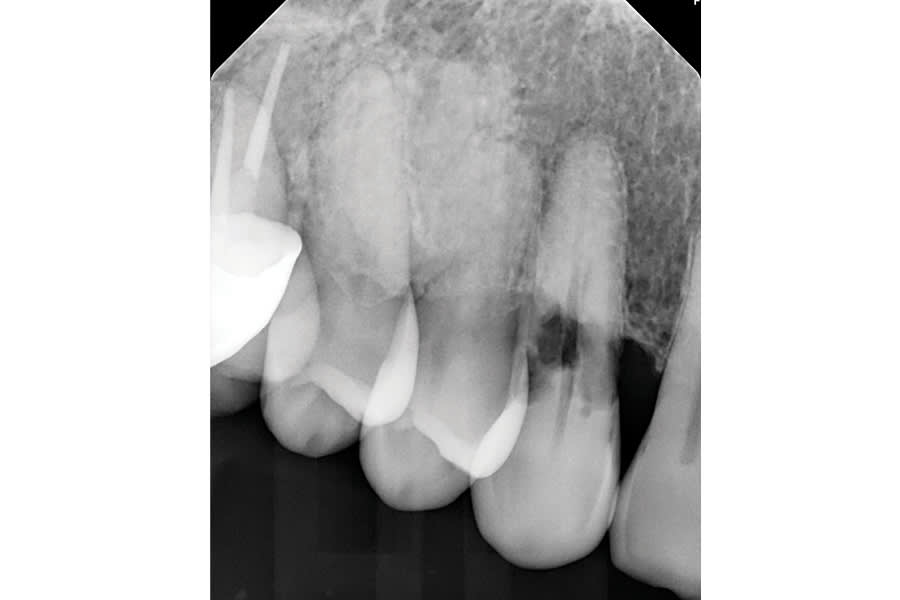
Figure 1

Figure 2

Figure 3

Figure 4

Figure 5
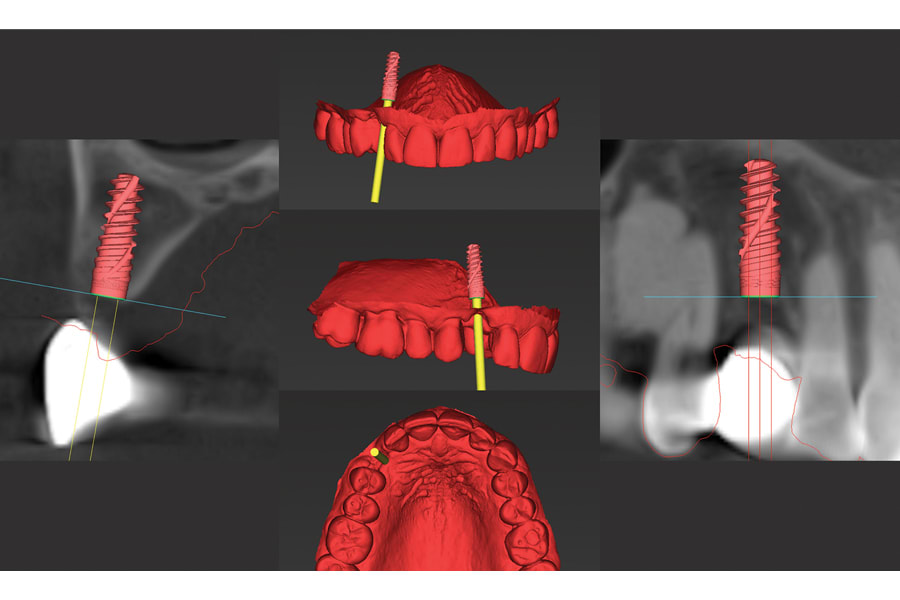
Figure 6

Figure 7

Figure 8

Figure 9

Figure 10
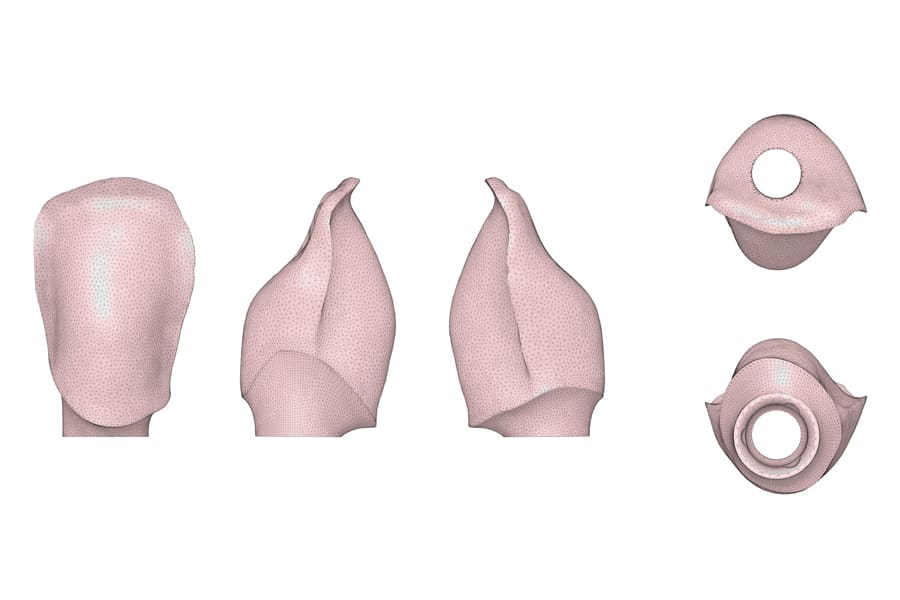
Figure 11

Figure 12

Figure 13

Figure 14

Figure 15